

The global, regional, and national burden of benign prostatic hyperplasia in 204 countries and territories from 2000 to 2019: a systematic analysis for the Global Burden of Disease Study 2019
- PMID: 36273485
- PMCID: PMC9640930
- DOI: 10.1016/S2666-7568(22)00213-6
The global, regional, and national burden of benign prostatic hyperplasia in 204 countries and territories from 2000 to 2019: a systematic analysis for the Global Burden of Disease Study 2019
Abstract
Background: Benign prostatic hyperplasia is a common urological disease affecting older men worldwide, but comprehensive data about the global, regional, and national burden of benign prostatic hyperplasia and its trends over time are scarce. As part of the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019, we estimated global trends in, and prevalence of, benign prostatic hyperplasia and disability-adjusted life-years (DALYs) due to benign prostatic hyperplasia, in 21 regions and 204 countries and territories from 2000 to 2019.
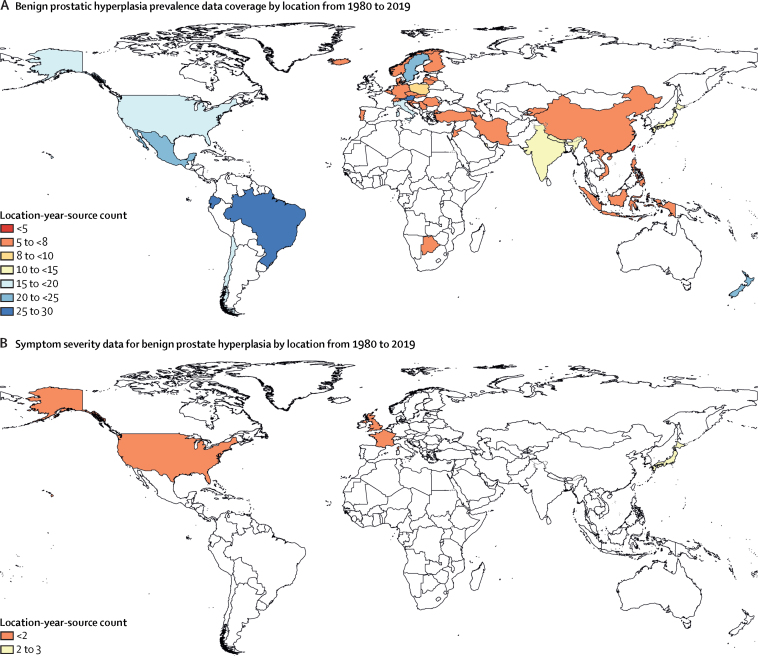
Methods: This study was conducted with GBD 2019 analytical and modelling strategies. Primary prevalence data came from claims from three countries and from hospital inpatient encounters from 45 locations. A Bayesian meta-regression modelling tool, DisMod-MR version 2.1, was used to estimate the age-specific, location-specific, and year-specific prevalence of benign prostatic hyperplasia. Age-standardised prevalence was calculated by the direct method using the GBD reference population. Years lived with disability (YLDs) due to benign prostatic hyperplasia were estimated by multiplying the disability weight by the symptomatic proportion of the prevalence of benign prostatic hyperplasia. Because we did not estimate years of life lost associated with benign prostatic hyperplasia, disability-adjusted life-years (DALYs) equalled YLDs. The final estimates were compared across Socio-demographic Index (SDI) quintiles. The 95% uncertainty intervals (UIs) were estimated as the 25th and 975th of 1000 ordered draws from a bootstrap distribution.
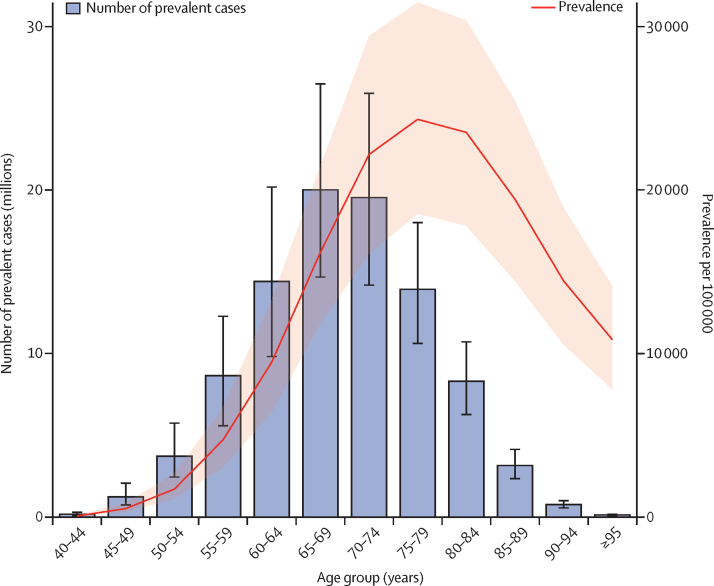
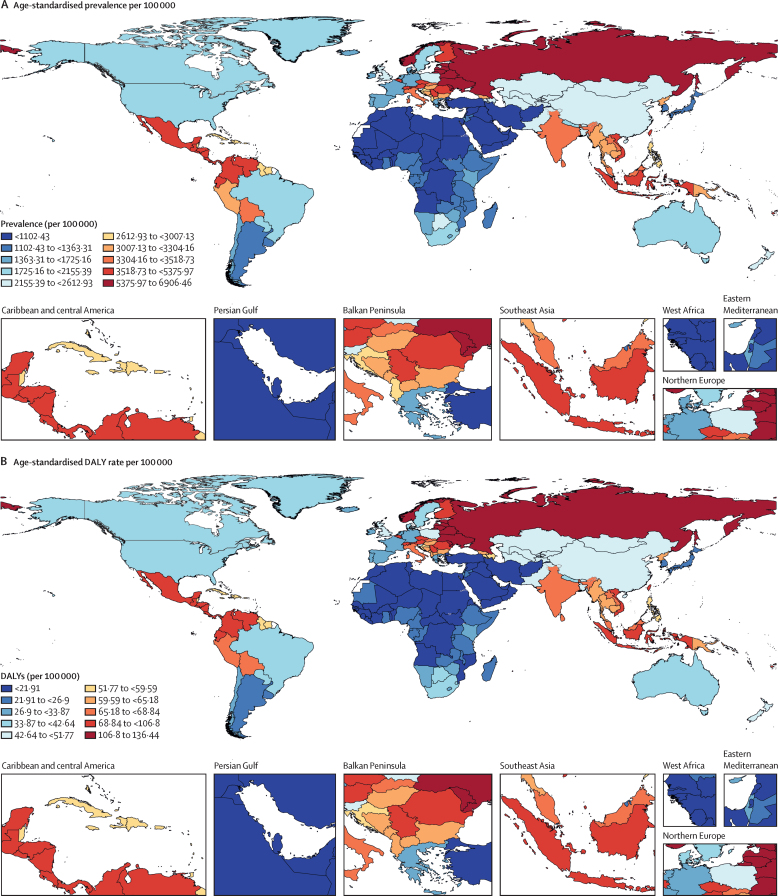
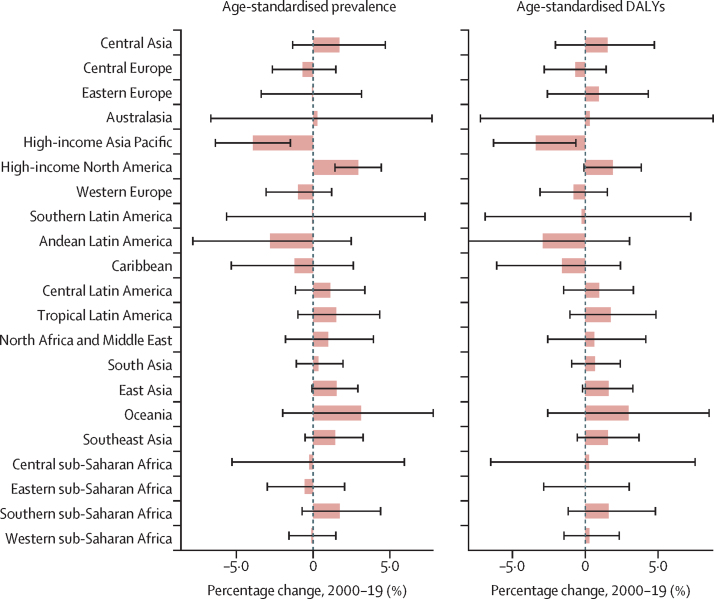
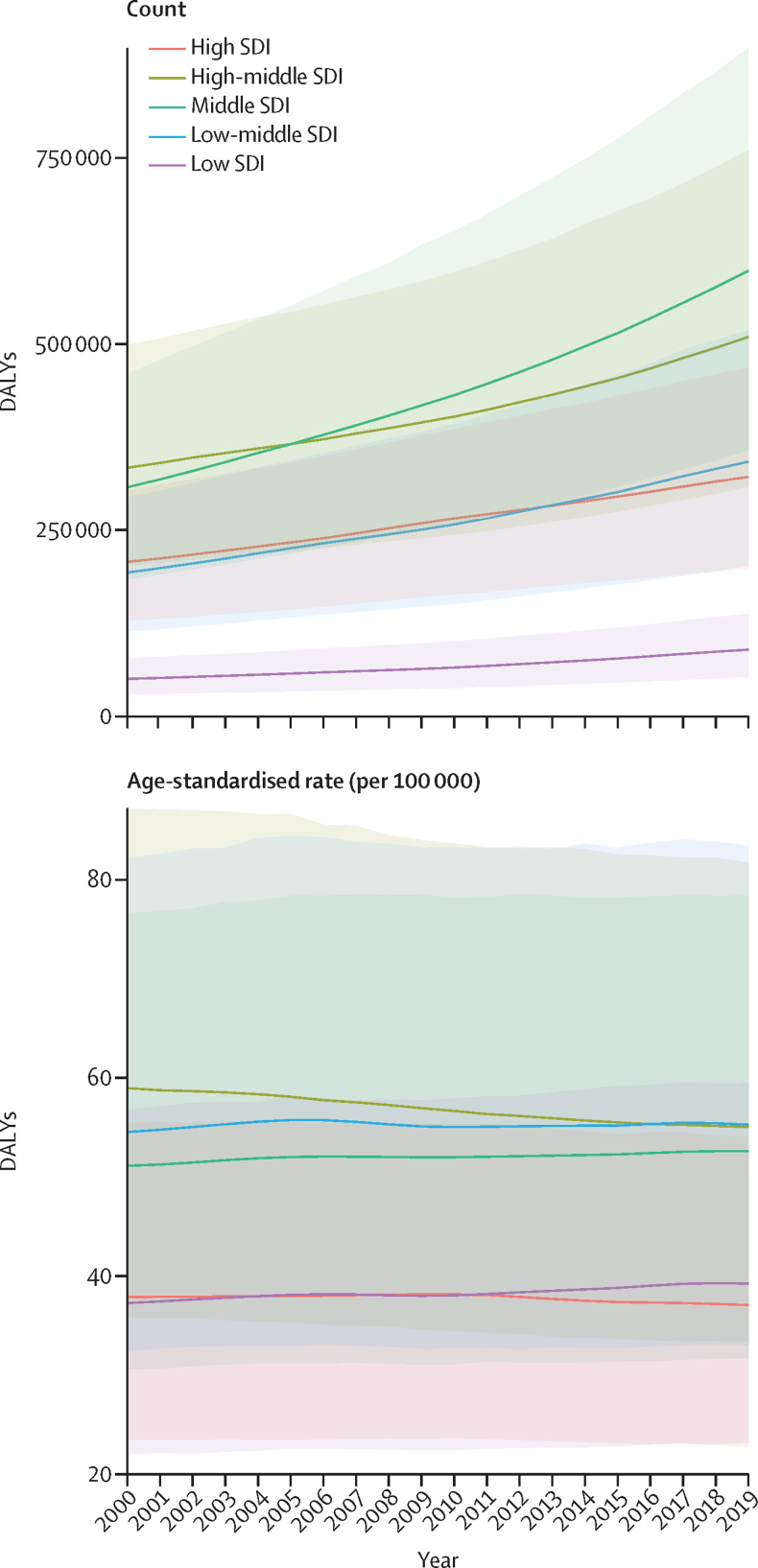
Findings: Globally, there were 94·0 million (95% UI 73·2 to 118) prevalent cases of benign prostatic hyperplasia in 2019, compared with 51·1 million (43·1 to 69·3) cases in 2000. The age-standardised prevalence of benign prostatic hyperplasia was 2480 (1940 to 3090) per 100 000 people. Although the global number of prevalent cases increased by 70·5% (68·6 to 72·7) between 2000 and 2019, the global age-standardised prevalence remained stable (-0·770% [-1·56 to 0·0912]). The age-standardised prevalence in 2019 ranged from 6480 (5130 to 8080) per 100 000 in eastern Europe to 987 (732 to 1320) per 100 000 in north Africa and the Middle East. All five SDI quintiles observed an increase in the absolute DALY burden between 2000 and 2019. The most rapid increases in the absolute DALY burden were seen in the middle SDI quintile (94·7% [91·8 to 97·6]), the low-middle SDI quintile (77·3% [74·1 to 81·2]), and the low SDI quintile (77·7% [72·9 to 83·2]). Between 2000 and 2019, age-standardised DALY rates changed less, but the three lower SDI quintiles (low, low-middle, and middle) saw small increases, and the two higher SDI quintiles (high and high-middle SDI) saw small decreases.
Interpretation: The absolute burden of benign prostatic hyperplasia is rising at an alarming rate in most of the world, particularly in low-income and middle-income countries that are currently undergoing rapid demographic and epidemiological changes. As more people are living longer worldwide, the absolute burden of benign prostatic hyperplasia is expected to continue to rise in the coming years, highlighting the importance of monitoring and planning for future health system strain.
Funding: Bill & Melinda Gates Foundation.
Translation: For the Amharic translation of the abstract see Supplementary Materials section.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests B Bikbov reports grants or contracts from the Lombardy Region outside the submitted work to their institution. T Garg reports support for attending meetings or travel from Siemens Healthineers outside the submitted work. N E Ismail reports unpaid leadership or fiduciary roles in board, society, committee, or advocacy groups with the Malaysian Academy of Pharmacy as a council member outside the submitted work. N Perico reports support for attending meetings or travel from and participation on a data safety monitoring board or advisory board with Bayer AG outside the submitted work. J A Singh reports consulting fees from Crealta Horizon, Medisys, Fidia, PK Med, Two Labs, Adept Field Solutions, Clinical Care Options, Clearview Healthcare Partners, Putnam Associates, Focus Forward, Navigant Consulting, Spherix, MedIQ, Jupiter Life Science, UBM, Trio Health, Medscape, WebMD, Practice Point Communications, the National Institutes of Health, and the American College of Rheumatology; payment or honoraria for lectures, presentations, speakers' bureaus, manuscript writing or educational events from Simply Speaking; support for attending meetings or travel from the steering committee of OMERACT; participation on a data safety monitoring board or advisory board with the US Food and Drug Administration Arthritis Advisory Committee; a leadership or fiduciary role in a board, society, committee or advocacy group, paid or unpaid, with OMERACT as a steering committee member, with the Veterans Affairs Rheumatology Field Advisory Committee as Chair (unpaid), and with the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis and editor and director (unpaid); stock or stock options in TPT Global Tech, Vaxart Pharmaceuticals, Atyu Biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics, Seres Therapeutics, Tonix Pharmaceuticals and Charlotte's Web Holdings; and having previously owned stock options in Amarin, Viking, and Moderna Pharmaceuticals, all outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Benign prostatic hyperplasia: a global challenge of the ageing population.Lancet Healthy Longev. 2022 Nov;3(11):e725-e726. doi: 10.1016/S2666-7568(22)00243-4. Epub 2022 Oct 20. Lancet Healthy Longev. 2022. PMID: 36273483 No abstract available.
References
-
- McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–1803. - PubMed
-
- Bushman W. Etiology, epidemiology, and natural history of benign prostatic hyperplasia. Urol Clin North Am. 2009;36:403–415. - PubMed
-
- Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132:474–479. - PubMed
-
- Kok ET, Schouten BW, Bohnen AM, Groeneveld FPMW, Thomas S, Bosch JLHR. Risk factors for lower urinary tract symptoms suggestive of benign prostatic hyperplasia in a community based population of healthy aging men: the Krimpen Study. J Urol. 2009;181:710–716. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
