Intercostal Nerve Cryoanalgesia Versus Thoracic Epidural Analgesia in Lung Transplantation: A Retrospective Single-Center Study
- PMID: 36274081
- PMCID: PMC9845479
- DOI: 10.1007/s40122-022-00448-z
Intercostal Nerve Cryoanalgesia Versus Thoracic Epidural Analgesia in Lung Transplantation: A Retrospective Single-Center Study
Abstract
Introduction: The optimal pain management strategy after lung transplantation is unknown. This study compared analgesic outcomes of intercostal nerve blockade by cryoanalgesia (Cryo) versus thoracic epidural analgesia (TEA).
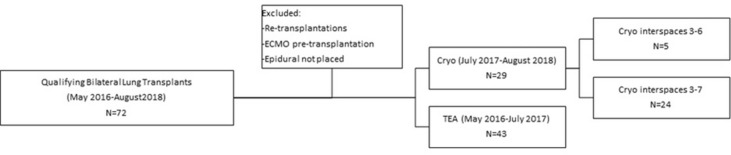
Methods: Seventy-two patients who underwent bilateral lung transplantation via clamshell incision at our center from 2016 to 2018 were managed with TEA (N = 43) or Cryo (N = 29). We evaluated analgesic-specific complications, opioid use in oral morphine equivalents (OME), and pain scores (0-10) through postoperative day 7. Adjusted linear regression was used to assess for non-inferiority of Cryo to TEA.
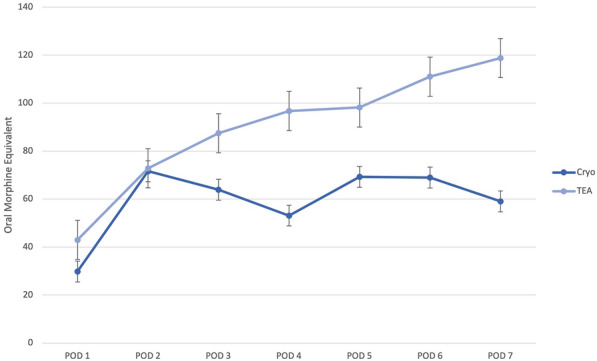
Results: The overall mean pain scores (Cryo 3.2 vs TEA 3.8, P = 0.21), maximum mean pain scores (Cryo 4.7 vs TEA 5.5, P = 0.16), and the total opioid use (Cryo 484 vs TEA 705 OME, P = 0.12) were similar in both groups, while the utilization of postoperative opioid-sparing analgesia, measured as use of lidocaine patches, was lower in the Cryo group (Cryo 21% vs TEA 84%, P < 0.001). Analgesic outcomes remained similar between the cohorts after adjustment for pertinent patient and analgesic characteristics (P = 0.26), as well as after exclusion of Cryo patients requiring rescue TEA (P = 0.32). There were no Cryo complications, with four patients requiring subsequent TEA for pain control. Two TEA patients experienced hemodynamic instability following a test TEA bolus requiring code measures. Additionally, TEA placement was delayed beyond postoperative day 1 in 33% owing to need for anticoagulation or clinical instability.
Conclusions: In lung transplantation, Cryo was found to be safe with analgesic effectiveness similar to TEA. Cryo may be advantageous in this complex patient population, as it can be used in all clinical scenarios and eliminates risks and delays associated with TEA.
Keywords: Bilateral thoracotomy; Cryoablation; Lung transplantation; Pain management; Thoracic epidural analgesia.
© 2022. The Author(s).
Figures