

Updated Perspectives on the Role of Biomechanics in COPD: Considerations for the Clinician
- PMID: 36274993
- PMCID: PMC9585958
- DOI: 10.2147/COPD.S339195
Updated Perspectives on the Role of Biomechanics in COPD: Considerations for the Clinician
Abstract
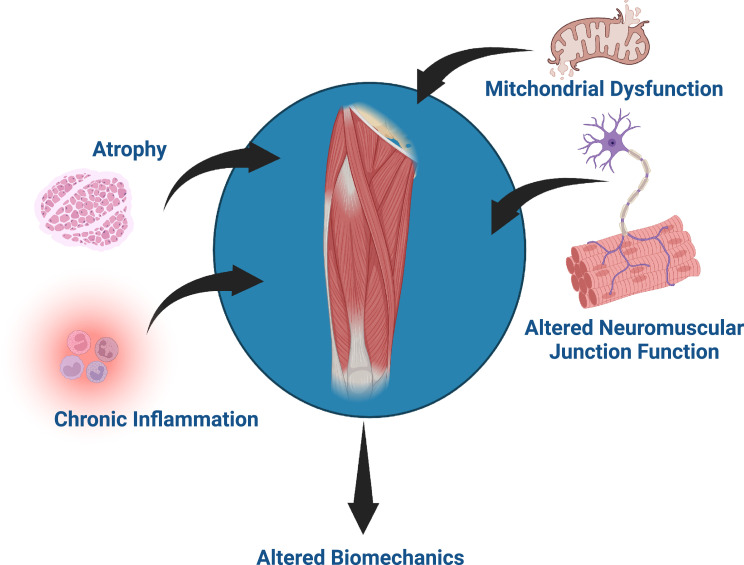
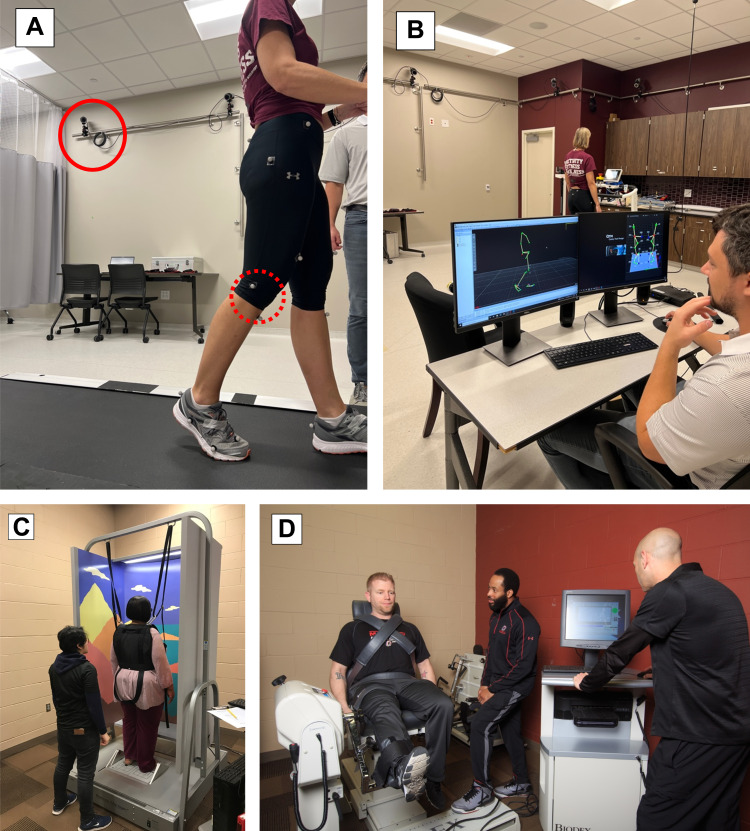
Patients with chronic obstructive pulmonary disease (COPD) demonstrate extra-pulmonary functional decline such as an increased prevalence of falls. Biomechanics offers insight into functional decline by examining mechanics of abnormal movement patterns. This review discusses biomechanics of functional outcomes, muscle mechanics, and breathing mechanics in patients with COPD as well as future directions and clinical perspectives. Patients with COPD demonstrate changes in their postural sway during quiet standing compared to controls, and these deficits are exacerbated when sensory information (eg, eyes closed) is manipulated. If standing balance is disrupted with a perturbation, patients with COPD are slower to return to baseline and their muscle activity is differential from controls. When walking, patients with COPD appear to adopt a gait pattern that may increase stability (eg, shorter and wider steps, decreased gait speed) in addition to altered gait variability. Biomechanical muscle mechanics (ie, tension, extensibility, elasticity, and irritability) alterations with COPD are not well documented, with relatively few articles investigating these properties. On the other hand, dyssynchronous motion of the abdomen and rib cage while breathing is well documented in patients with COPD. Newer biomechanical technologies have allowed for estimation of regional, compartmental, lung volumes during activity such as exercise, as well as respiratory muscle activation during breathing. Future directions of biomechanical analyses in COPD are trending toward wearable sensors, big data, and cloud computing. Each of these offers unique opportunities as well as challenges. Advanced analytics of sensor data can offer insight into the health of a system by quantifying complexity or fluctuations in patterns of movement, as healthy systems demonstrate flexibility and are thus adaptable to changing conditions. Biomechanics may offer clinical utility in prediction of 30-day readmissions, identifying disease severity, and patient monitoring. Biomechanics is complementary to other assessments, capturing what patients do, as well as their capability.
Keywords: balance; kinematics; kinetics; mechanomyography; postural control; wearables.
© 2022 Yentes et al.
Conflict of interest statement
Dr Stephen I Rennard reports personal fees from BoehringerIngelheim, GSK, Sanofi, and Verona. Dr Stephen I Rennard is the founder and president of Great Plains Biometrix and Drs. Jennifer M Yentes and Eric Markvicka sit on the Board of Directors, outside the submitted work. In addition, Drs. Jennifer M Yentes and Stephen I Rennard have a patent for gait respiratory coupling issued and licensed by UNeMed, and a patent wearable multifunction sensor pending with Dr. Eric Markvicka. The authors report no other conflicts of interest in this work.
Figures
Comment in
-
Updated Perspectives on the Role of Biomechanics in COPD: Considerations for the Clinician [Letter].Int J Chron Obstruct Pulmon Dis. 2022 Nov 30;17:3017-3018. doi: 10.2147/COPD.S395493. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 36475040 Free PMC article. No abstract available.
Similar articles
-
Subjects With COPD Walk With Less Consistent Organization of Movement Patterns of the Lower Extremity.Respir Care. 2020 Feb;65(2):158-168. doi: 10.4187/respcare.06743. Epub 2019 Nov 12. Respir Care. 2020. PMID: 31719193 Free PMC article.
-
Gait mechanics in patients with chronic obstructive pulmonary disease.Respir Res. 2015 Feb 28;16(1):31. doi: 10.1186/s12931-015-0187-5. Respir Res. 2015. PMID: 25849481 Free PMC article.
-
Gait deficiencies associated with peripheral artery disease are different than chronic obstructive pulmonary disease.Gait Posture. 2017 Sep;57:258-264. doi: 10.1016/j.gaitpost.2017.06.018. Epub 2017 Jun 27. Gait Posture. 2017. PMID: 28683417 Free PMC article.
-
Gait differences between COPD and healthy controls: systematic review and meta-analysis.Eur Respir Rev. 2024 Apr 24;33(172):230253. doi: 10.1183/16000617.0253-2023. Print 2024 Apr 30. Eur Respir Rev. 2024. PMID: 38657998 Free PMC article.
-
Gait characteristics and falls in Parkinson's disease: A systematic review and meta-analysis.Parkinsonism Relat Disord. 2018 Dec;57:1-8. doi: 10.1016/j.parkreldis.2018.07.008. Epub 2018 Jul 17. Parkinsonism Relat Disord. 2018. PMID: 30041848
Cited by
-
Analysis of emerging trends and hot spots in respiratory biomechanics from 2003 to 2022 based on CiteSpace.Front Physiol. 2023 Jul 20;14:1190155. doi: 10.3389/fphys.2023.1190155. eCollection 2023. Front Physiol. 2023. PMID: 37546534 Free PMC article.
-
Balance, gait, and postural control impairment and fall risk in patients with chronic obstructive pulmonary disease and breathing pattern disorder: A case-control study.Medicine (Baltimore). 2025 Aug 8;104(32):e43609. doi: 10.1097/MD.0000000000043609. Medicine (Baltimore). 2025. PMID: 40797477 Free PMC article.
-
Updated Perspectives on the Role of Biomechanics in COPD: Considerations for the Clinician [Letter].Int J Chron Obstruct Pulmon Dis. 2022 Nov 30;17:3017-3018. doi: 10.2147/COPD.S395493. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 36475040 Free PMC article. No abstract available.
-
Applicability of the Instrumented Pendulum Test for Assessing Limb Viscoelastic Properties in Neurological and Internal Diseases: A Narrative Review.Life (Basel). 2025 Mar 24;15(4):535. doi: 10.3390/life15040535. Life (Basel). 2025. PMID: 40283090 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
