

Missed anti-D immune globulin administration to postpartum patients in 2 health systems: an unrecognized patient safety risk
- PMID: 36275497
- PMCID: PMC9563491
- DOI: 10.1016/j.xagr.2021.100038
Missed anti-D immune globulin administration to postpartum patients in 2 health systems: an unrecognized patient safety risk
Abstract
Background: Maternal-fetal Rh-alloimmunization is a rare but potentially fatal event, most often caused by maternal exposure to D-antigen-presenting Rh-positive erythrocytes at the time of delivery. Prophylaxis with anti-D immune globulin is highly effective with a low side-effect profile and results in a dramatically decreased risk of alloimmunization. Postpartum anti-D immune globulin prophylaxis is recommended by national societies to reduce Rh-alloimmunization. We hypothesized that a small number of postpartum patients do not receive prophylaxis as indicated. .
Objective: We investigated patients in 2 separate health systems that did not receive indicated prophylaxis and devised a suite of Electronic Health Record interventions to prevent future errors.
Study design: We reviewed charts retrospectively from Electronic Health Record data of 2 urban academic health systems, the MetroHealth System and Oregon Health & Science University. We identified all Rh-negative postpartum patients and their infants delivering from 2014 to 2019. The primary outcome was the proportion of postpartum patients not receiving indicated anti-D immune globulin prophylaxis. Once cases of missed anti-D immune globulin prophylaxis were identified, we reviewed individual charts to determine the relevant clinical circumstances and potential causes for error.
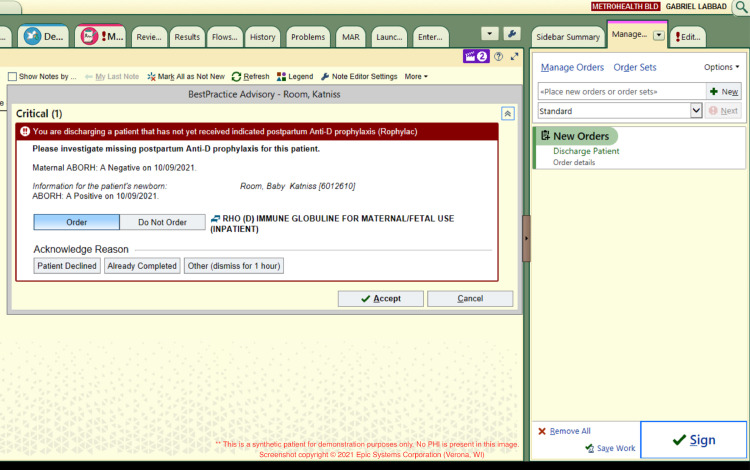
Results: Of 29,801 deliveries over 5 years (15,444 at MetroHealth System and 14,357 at Oregon Health & Science University), there were 3087 Rh-negative postpartum patients, of whom 7 were alloimmunized and ineligible for prophylaxis. Anti-D immune globulin was indicated for 2162 (70.0%) women as they delivered an Rh-positive infant. A total of 37 indicated patients did not receive postpartum anti-D immune globulin. Twenty patients were offered prophylaxis and declined. We missed a total of 17 opportunities, thus our institutions appropriately offered indicated anti-D prophylaxis to 99.2% of patients over a period of 5 years. Of the 17 true misses, anti-D immune globulin was ordered for some patients, whereas others did not have an anti-D immune globulin order placed. A toolkit in the Electronic Health Record consisting of decision-support hard stops, automated documentation, and longitudinal reporting was implemented at the MetroHealth System in the year after its inception. The Toolkit identified and helped prevent 4 potential misses, resulting in a 100% anti-D prophylaxis rate at the MetroHealth System.
Conclusion: Given the serious nature of Rh-alloimmunization, we believe missed prophylaxis should be a never event. Through examination of our current processes, we identified areas of improvement and developed a Postpartum Anti-D Immune Globulin Prophylaxis Electronic Health Record Toolkit, which showed improvement in administration rates. Such a toolkit has the potential to identify patients appropriately and avoid missed anti-D immune globulin prophylaxis events.
Keywords: anti-D immunoglobulin; electronic health record toolkit; maternal-fetal alloimmunization; missed prophylaxis; never event; obstetrical informatics; obstetrical quality improvement; rhesus immunoglobulin prophylaxis.
© 2021 The Authors.
Figures



References
-
- Kumpel BM. On the immunologic basis of Rh immune globulin (anti-D) prophylaxis. Transfusion. 2006;46:1652–1656. - PubMed
-
- Bowman JM. Controversies in Rh prophylaxis. Who needs Rh immune globulin and when should it be given? Am J Obstet Gynecol. 1985;151:289–294. - PubMed
-
- Bowman JM. The prevention of Rh immunization. Transfus Med Rev. 1988;2:129–150. - PubMed
-
- Badami KG, Parker J, Kenny A, Warrington S. Incidence of maternal sensitisation to Rh(D) in Christchurch, New Zealand and reasons for prophylaxis failures. N Z Med J. 2014;127:40–46. - PubMed
-
- MacKenzie IZ, Bichler J, Mason GC, et al. Efficacy and safety of a new, chromatographically purified rhesus (D) immunoglobulin. Eur J Obstet Gynecol Reprod Biol. 2004;117:154–161. - PubMed
LinkOut - more resources
Full Text Sources
