

Posteromedial Tibial Bone Bruise After Anterior Cruciate Ligament Injury: An MRI Study of Bone Bruise Patterns in 208 Patients
- PMID: 36276425
- PMCID: PMC9580091
- DOI: 10.1177/23259671221120636
Posteromedial Tibial Bone Bruise After Anterior Cruciate Ligament Injury: An MRI Study of Bone Bruise Patterns in 208 Patients
Abstract
Background: Bone bruise patterns after anterior cruciate ligament (ACL) rupture may predict the presence of intra-articular pathology and help explain the mechanism of injury. Lateral femoral condyle (LFC) and lateral tibial plateau (LTP) bone bruises are pathognomic to ACL rupture. There is a lack of information regarding medial tibial plateau (MTP) and medial femoral condyle (MFC) bone bruises.
Purpose: To summarize the prevalence and location of MTP bone bruises with acute ACL rupture and to determine the predictors of MTP bone bruises.
Study design: Cross-sectional study; Level of evidence, 3.
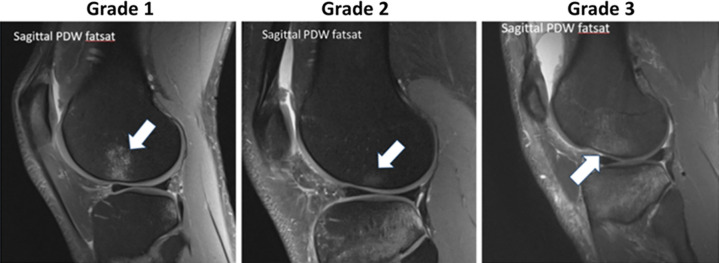
Methods: Inclusion criteria were patients who underwent ACL reconstruction between February 2015 and November 2017, magnetic resonance imaging (MRI) within 90 days of injury, and participation in the database. Exclusion criteria included previous ipsilateral surgery, multiligamentous injuries, and incomplete imaging. Due to the large number of cases remaining (n = 600), 150 patients were selected randomly from each year included in the study, for a total of 300 patients. Two readers independently reviewed injury MRI scans using the Costa-Paz bone bruise grading system. Logistic regression was used to identify factors associated with MTP bone bruises.
Results: Included were 208 patients (mean age, 23.8 years; mean body mass index, 25.6). The mechanism of injury was noncontact in 59% of injuries, with over half from soccer, basketball, and football. The median time from injury to MRI scan was 12 days. Of the 208 patients, 98% (203/208) had a bone bruise, 79% (164/208) had an MTP bone bruise, and 83% (172/208) had bruises in both medial and lateral compartments. The most common pattern, representing 46.6% of patients (97/208), was a bruise in all 4 locations (MFC, LFC, MTP, and LTP). Of the 164 MTP bruises, 160 (98%) involved the posterior third of the plateau, and 161 were grade 1. The presence of an MFC bruise was the only independent risk factor for an MTP bruise (odds ratio, 3.71). The resulting nomogram demonstrated MFC bruise, sport, and mechanism of injury were the most important predictors of an MTP bruise.
Conclusion: MTP bruise after acute ACL rupture was as prevalent as lateral bruises. The presence of a posterior MTP bruise suggested anterior tibial translation at the time of injury and could portend more medial compartment pathology at the time of injury than previously recognized.
Keywords: anterior cruciate ligament rupture; bone bruise; bone marrow pattern.
© The Author(s) 2022.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: C.W. has received research support from Janssen Research and Development and consulting fees from Siemens Medical Solutions. L.D.F. has received hospitality payments from DJO. A.A.M. has received education payments from Arthrex; consulting fees from Amniox Medical, Anika Therapeutics, Arthrosurface, Trice Medical, and Zimmer Biomet; speaking fees, royalties, and honoraria from Arthrosurface; and stock options from Anika Therapeutics. J.T.R. has received speaking fees from Smith & Nephew. P.M.S. has received consulting fees and speaking fees from Arthrex and honoraria from NovoPedics. K.P.S. has received research support from DJO and Smith & Nephew and consulting fees from Flexion Therapeutics, the National Football League, and Novopeds. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures



References
-
- Ali A, Pillai J, Gulati V, Gibbons C, Roberton B. Hyperextension injuries of the knee: do patterns of bone bruising predict soft tissue injury? Skeletal Radiol. 2018;47(2):173–179. - PubMed
-
- Costa-Paz M, Muscolo DL, Ayerza M, Makino A, Aponte-Tinao L. Magnetic resonance imaging follow-up study of bone bruises associated with anterior cruciate ligament ruptures. Arthroscopy. 2001;17(5):445–449. - PubMed
-
- Davies NH, Niall D, King LJ, Lavelle J, Healy JC. Magnetic resonance imaging of bone bruising in the acutely injured knee–-short-term outcome. Clin Radiol. 2004;59(5):439–445. - PubMed
-
- Faber KJ, Dill JR, Amendola A, et al. Occult osteochondral lesions after anterior cruciate ligament rupture. Am J Sports Med. 1999;27(4):489–494. - PubMed
LinkOut - more resources
Full Text Sources
