

Diagnostic challenges and treatment options in patients with solitary fibrous tumor: A single-center observational study
- PMID: 36277294
- PMCID: PMC9583656
- DOI: 10.3389/fsurg.2022.952463
Diagnostic challenges and treatment options in patients with solitary fibrous tumor: A single-center observational study
Abstract
Introduction: Solitary fibrous tumor (SFT) is an extremely rare disease with a high misdiagnosis rate and a potentially malignant biologic nature. We have collected and analyzed data from 18 SFT patients to provide a deeper insight into this uncommon disease entity.
Methods: In our study, 18 patients who had undergone surgery between April 2014 and December 2021 for the diagnosis of SFT were evaluated. The collected data for each patient included the location of the SFT, the preoperative diagnosis, the definitive histological diagnosis, the presence of postoperative complications, the time of recurrence, the time of systemic progression, the type of treatment, and the survival rate. The median follow-up was 36 months.
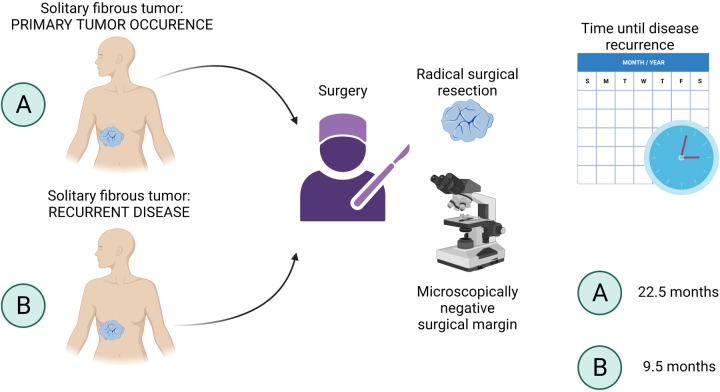
Results: In three patients, the preoperative diagnosis did not correlate with the definitive histology of SFT. In patients with the limb location of SFT, no signs of recurrence nor distant metastases were seen within the study period. In total, 50% of the postsurgical complications were associated with the abdominal location of the SFT. In newly diagnosed SFT patients, two patients (20%) developed local recurrence, and the median time until recurrence was 22.5 months. Out of patients that were admitted and operated on for recurrent SFT, 67% relapsed, and the median time to relapse was 9.5 months. The systemic progression of the disease was observed in 33% of patients treated for recurrent SFT.
Conclusion: In our study, the misdiagnosis rate was high and correlated with previously published studies. Postsurgical complications were associated with the extrathoracic location of SFT. The mainstay of SFT treatment remains radical surgery, although radiotherapy alone can significantly improve overall survival. Clinical trials are urgently needed to evaluate the potential effect of other treatment modalities, such as immunotherapy and targeted therapy, in SFT patients.
Keywords: SFT metastasis; SFT surgery; SFT surgical complications; SFT treatment; soft tissue sarcoma, pseudosarcomatous lesions, sarcoma misdiagnosis, solitary fibrous tumor recurrence.
© 2022 Ozaniak, Hladik, Lischke and Strizova.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources
Miscellaneous