

Gestational diabetes is associated with alteration on pelvic floor muscle activation pattern during pregnancy and postpartum: Prospective cohort using electromyography assessment
- PMID: 36277705
- PMCID: PMC9582526
- DOI: 10.3389/fendo.2022.958909
Gestational diabetes is associated with alteration on pelvic floor muscle activation pattern during pregnancy and postpartum: Prospective cohort using electromyography assessment
Abstract
Background and objective: Gestational diabetes mellitus (GDM) is a comorbidity which may cause acute and lifelong disorders to mother and child. Alterations in muscular and connective tissues have been associated with GDM in translation studies, characterizing gestational diabetic myopathy. Pregnancy-specific urinary incontinence and sexual disabilities, disorders that depend on the pelvic floor muscle (PFM) integrity, are also associated with GDM both during and after pregnancy. The aim was to compare PFM activation patterns between GDM and non-GDM women from 24-30 gestational weeks to 18-24 months postpartum during a standard clinical test during gestation and postpartum.
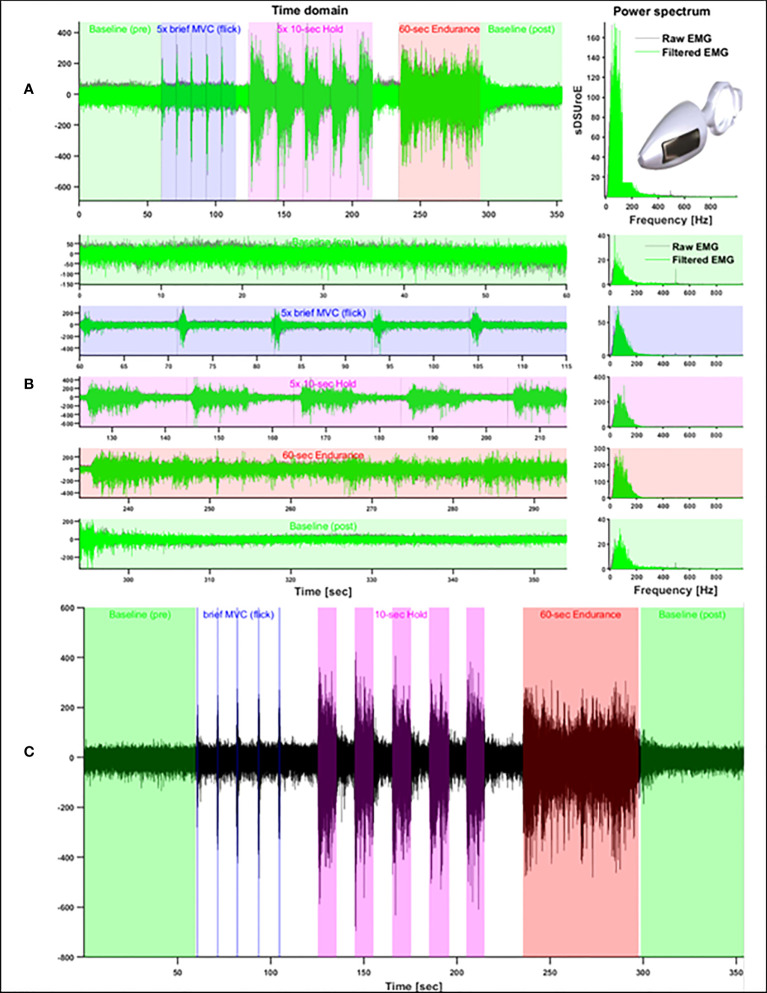
Methods: We conducted a prospective three-time-point cohort study from gestation (24-30 weeks-T1, and 36-38 weeks-T2) to 18-24 months postpartum (T3). PFM electromyography was recorded in primigravida or primiparous women with one previous elective c-section with or without the diagnosis of GDM according to the American Diabetes Association criteria. A careful explanation of the muscle anatomy and functionality of the PFM was given to participants before EMG assessment. The outcome measures were PFM activation patterns assessed during pregnancy and postpartum, comparing intra and between groups. PFM activation patterns were assessed by normalized electromyography signal at rest and during 1-second (sec) phasic, 10-sec hold, and 60-sec sustained contractions.
Results: Demographic and obstetric data showed homogeneity between groups. The GDM group achieved peak PFM EMG amplitudes similarly to the non-GDM group, but they took longer to return to baseline levels during the ~1-sec contraction (flicks). During 10-sec hold contractions, the GDM group sustained lower levels of PFM activation than the non-GDM group at both 36-38 weeks of gestation and 18-24 months postpartum when compared to the non-GDM group.
Conclusion: The results suggest that GDM impaired PFM control mainly on 1-sec flicks and 10-sec hold contraction, which appears to develop during late pregnancy and extends long-term postpartum. This motor behavior may play a role on pelvic floor dysfunctions.
Keywords: electromyography; gestational diabetes; pelvic floor; postpartum; pregnant.
Copyright © 2022 Prudencio, Nunes, Pinheiro, Sartorão Filho, Nava, Salomoni, Pedroni, Rudge, Barbosa and Diamater Study Group.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Piculo F, Marini G, Vesentini G, Morceli G, Damasceno DC, Sobrevia L, et al. Pregnancy-specific urinary incontinence in women with gestational hyperglycaemia worsens the occurrence and severity of urinary incontinence and quality of life over the first year post partum. Eur J Obstet Gynecol Reprod Biol (2020) 252:336–43. doi: 10.1016/j.ejogrb.2020.06.036 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical