

Clinical efficacy and safety of ultrasound-assisted thrombolysis vs. standard catheter-directed thrombolysis in patients with acute pulmonary embolism: A study level meta-analysis of clinical trials
- PMID: 36277787
- PMCID: PMC9581227
- DOI: 10.3389/fcvm.2022.967786
Clinical efficacy and safety of ultrasound-assisted thrombolysis vs. standard catheter-directed thrombolysis in patients with acute pulmonary embolism: A study level meta-analysis of clinical trials
Abstract
Aim: To compare the clinical efficacy of ultrasound-assisted thrombolysis (USAT) vs. standard catheter-directed thrombolysis (SCDT) in patients with acute pulmonary embolism (aPE).
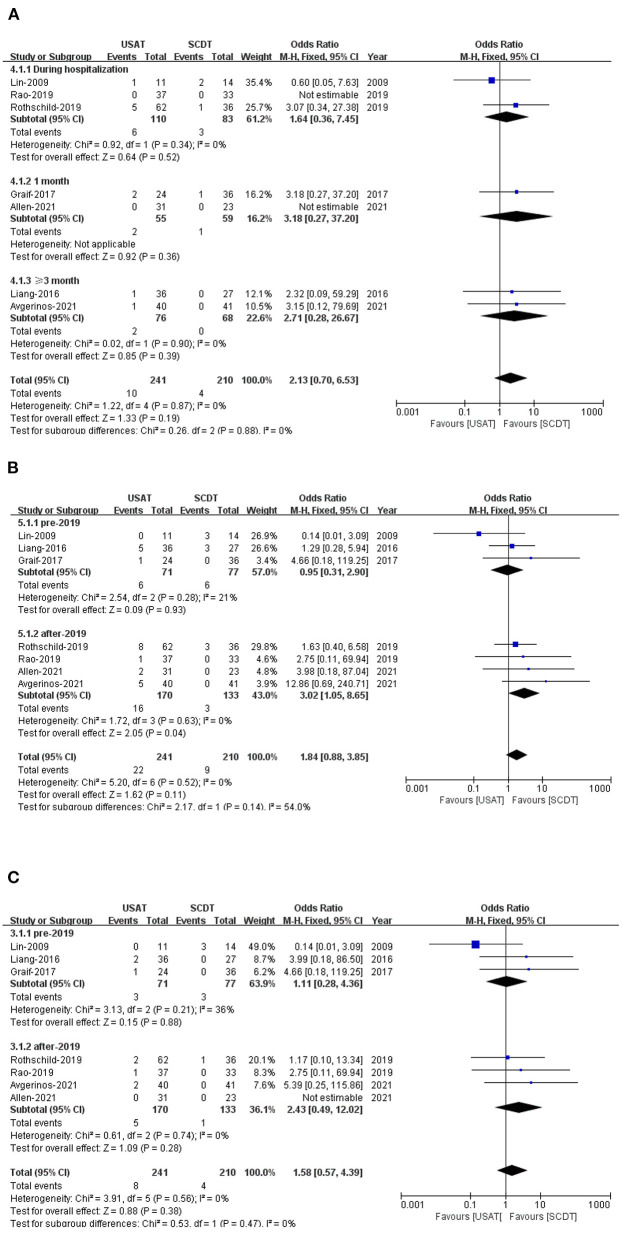
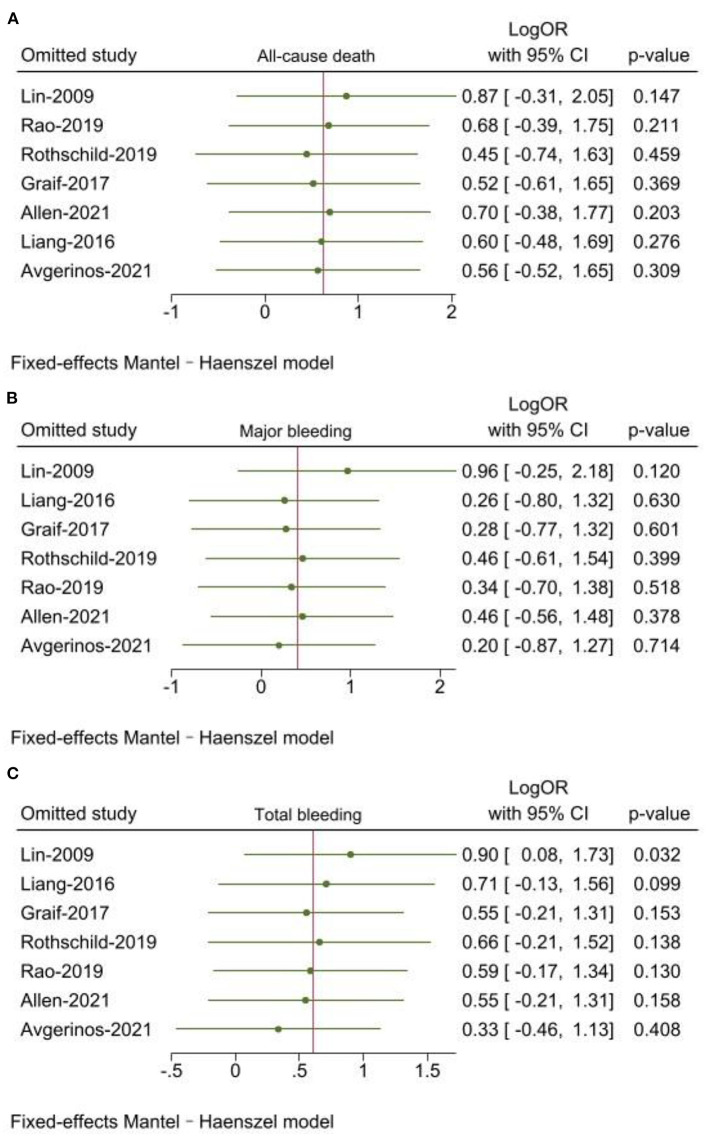
Methods: This study analyzed the clinical outcomes of patients with non-low-risk aPE who received USAT or SCDT. The primary outcomes were all-cause death, total bleeding, and major bleeding. Secondary outcomes included pulmonary thrombotic load score (Miller), improvement in right ventricular-to-left ventricular ratio (RV/LV), dose and duration of the thrombolytic drug tissue plasminogen activator (tPA), length of stay (LOS) in the ICU, and total LOS in the hospital.
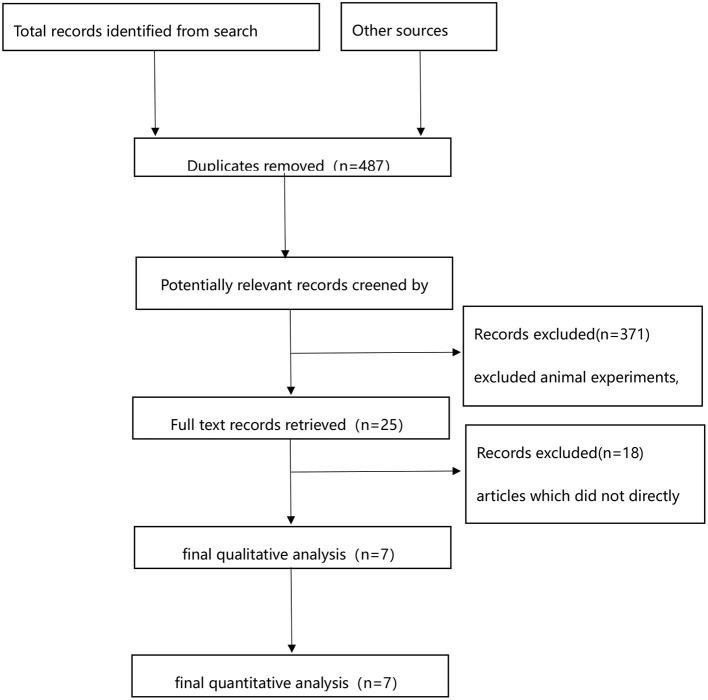
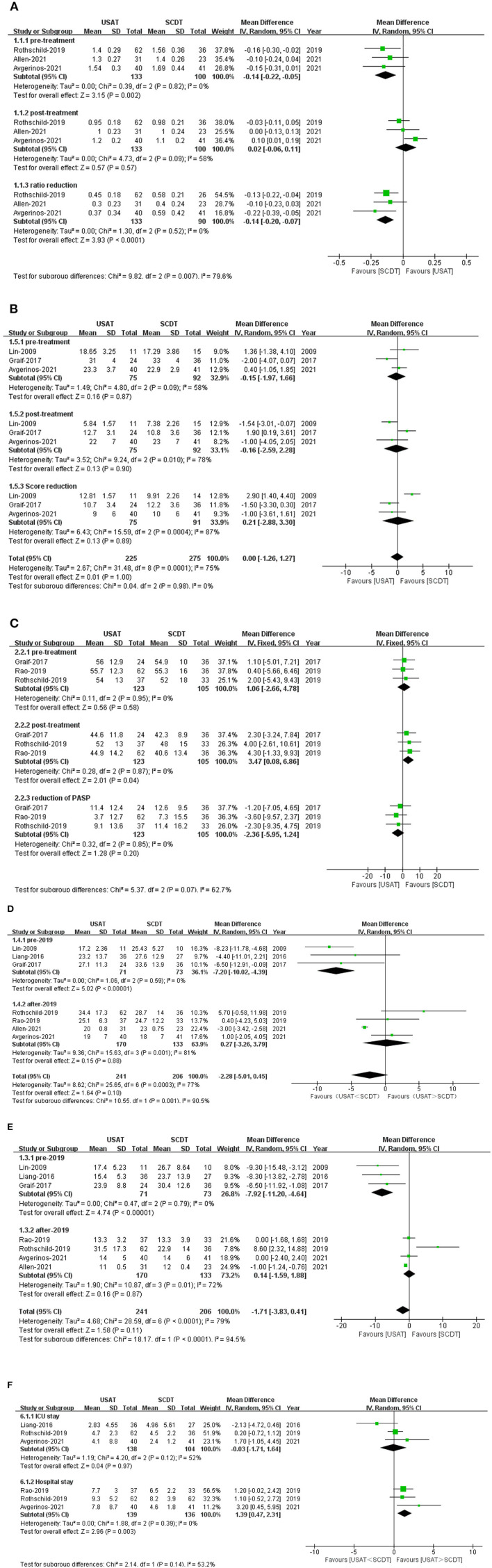
Results: A total of seven articles and 451 patients were included in this study. 241 patients were in the USAT group and 210 patients were in the SCDT group. There were no significant differences in all-cause mortality, total bleeding, and major bleeding between the two groups. Miller scores for pulmonary thrombus also showed no difference between the two groups, but pulmonary artery systolic pressure (PASP) was lower in the SCDT group after-treatment. The reduction of RV/LV from baseline was more pronounced in the SCDT group than in the USAT group (OR: -0.14, 95%CI: -0.20 to 0.07, P < 0.0001, I 2 = 0%). Total dose of tPA and duration of infusion in the USAT group were lower than those in the SCDT group, but there was no significant statistical difference. LOS in the ICU was similar between the two groups, while LOS in the hospital was lower in the SCDT group.
Conclusion: This study did not detect any differences in all-cause mortality, total bleeding, and major bleeding between non-low-risk aPE patients treated with USAT or SCDT. Improvement in right ventricular function was better in the SCDT group, and hospital LOS was lower in the SCDT group.
Keywords: acute pulmonary embolism; catheter-directed thrombolysis; standard catheter-directed thrombolysis; tissue plasminogen activator; ultrasound-assisted thrombolysis.
Copyright © 2022 Sun, Yang, Wang, Zhou, Chu, Li and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Ultrasound-Assisted Versus Standard Catheter-Directed Thrombolysis for Acute Pulmonary Embolism: Insights From National Inpatient Sample.J Soc Cardiovasc Angiogr Interv. 2024 Apr 5;3(5):101360. doi: 10.1016/j.jscai.2024.101360. eCollection 2024 May. J Soc Cardiovasc Angiogr Interv. 2024. PMID: 39132462 Free PMC article.
-
Comparison of safety and efficacy of ultrasound-accelerated thrombolysis vs. standard catheter-directed thrombolysis for the management of acute pulmonary embolism - a systematic review and meta-analysis.J Thromb Thrombolysis. 2025 Jun;58(5):623-635. doi: 10.1007/s11239-025-03100-7. Epub 2025 Apr 26. J Thromb Thrombolysis. 2025. PMID: 40281265
-
Randomized Trial Comparing Standard Versus Ultrasound-Assisted Thrombolysis for Submassive Pulmonary Embolism: The SUNSET sPE Trial.JACC Cardiovasc Interv. 2021 Jun 28;14(12):1364-1373. doi: 10.1016/j.jcin.2021.04.049. JACC Cardiovasc Interv. 2021. PMID: 34167677 Free PMC article. Clinical Trial.
-
Comparison of the Clinical Efficacy and Safety of Standard and Ultrasound-Assisted Thrombolysis for Pulmonary Embolism: A Systematic Review and Meta-Analysis.J Endovasc Ther. 2025 Jun;32(3):558-566. doi: 10.1177/15266028231181031. Epub 2023 Jun 8. J Endovasc Ther. 2025. PMID: 37291849
-
A Meta-analysis of Standard Versus Ultrasound-Assisted Catheter-Directed Thrombolysis in the Management of Acute Pulmonary Embolism.J Soc Cardiovasc Angiogr Interv. 2023 Jan 4;2(1):100514. doi: 10.1016/j.jscai.2022.100514. eCollection 2023 Jan-Feb. J Soc Cardiovasc Angiogr Interv. 2023. PMID: 39132529 Free PMC article. Review.
Cited by
-
Ultrasound-Assisted Versus Standard Catheter-Directed Thrombolysis for Acute Pulmonary Embolism: Insights From National Inpatient Sample.J Soc Cardiovasc Angiogr Interv. 2024 Apr 5;3(5):101360. doi: 10.1016/j.jscai.2024.101360. eCollection 2024 May. J Soc Cardiovasc Angiogr Interv. 2024. PMID: 39132462 Free PMC article.
-
Assessment of effectiveness and safety of thrombolytic therapy to pulmonary emboli by endobronchial ultrasound-guided transbronchial needle injection.JTCVS Tech. 2023 Sep 20;22:292-304. doi: 10.1016/j.xjtc.2023.09.005. eCollection 2023 Dec. JTCVS Tech. 2023. PMID: 38152238 Free PMC article.
-
Response to Letter to the Editor regarding the article "Comparison of Large-Bore Thrombectomy With Catheter-Directed Thrombolysis for the Treatment of Pulmonary Embolism".J Soc Cardiovasc Angiogr Interv. 2023 May 16;2(4):101034. doi: 10.1016/j.jscai.2023.101034. eCollection 2023 Jul-Aug. J Soc Cardiovasc Angiogr Interv. 2023. PMID: 39131631 Free PMC article. No abstract available.
-
Comparison of safety and efficacy of ultrasound-accelerated thrombolysis vs. standard catheter-directed thrombolysis for the management of acute pulmonary embolism - a systematic review and meta-analysis.J Thromb Thrombolysis. 2025 Jun;58(5):623-635. doi: 10.1007/s11239-025-03100-7. Epub 2025 Apr 26. J Thromb Thrombolysis. 2025. PMID: 40281265
References
-
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, et al. . 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): the task force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J. (2019) 54:1901647. 10.1183/13993003.01647-2019 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous