

Estimating the Prevalence of Dementia and Mild Cognitive Impairment in the US: The 2016 Health and Retirement Study Harmonized Cognitive Assessment Protocol Project
- PMID: 36279130
- PMCID: PMC9593315
- DOI: 10.1001/jamaneurol.2022.3543
Estimating the Prevalence of Dementia and Mild Cognitive Impairment in the US: The 2016 Health and Retirement Study Harmonized Cognitive Assessment Protocol Project
Abstract
Importance: Nationally representative data are critical for understanding the causes, costs, and outcomes associated with dementia and mild cognitive impairment (MCI) in the US and can inform policies aimed at reducing the impact of these conditions on patients, families, and public programs. The nationally representative Health and Retirement Study (HRS) is an essential resource for such data, but the HRS substudy providing dementia diagnostic information was fielded more than 20 years ago and more recent data are needed.
Objective: The Harmonized Cognitive Assessment Protocol (HCAP) was developed to update national estimates of the prevalence of MCI and dementia in the US and examine differences by age, race, ethnicity, and sex.
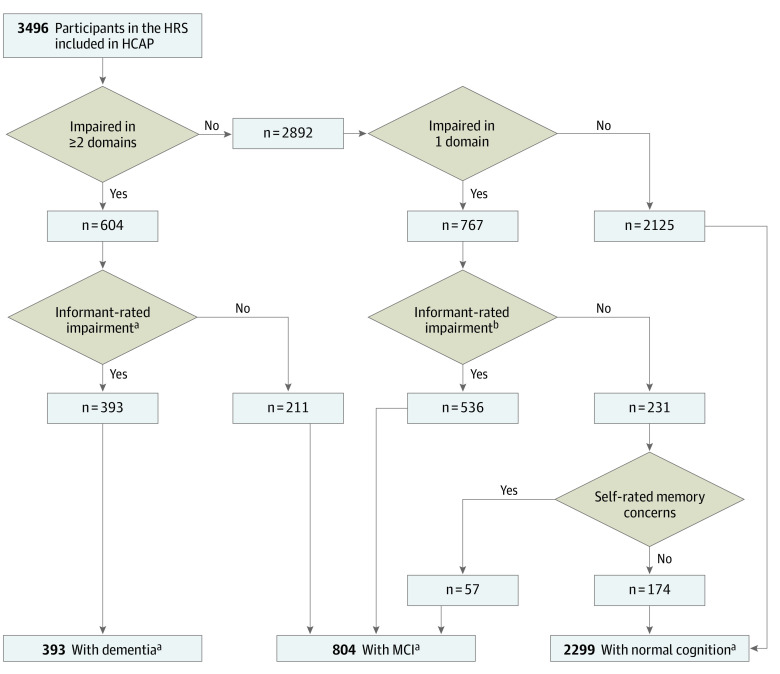
Design, setting, and participants: HRS is an ongoing longitudinal nationally representative study of people 51 years and older with staggered entry dates from 1992 to 2022 and follow-up ranging from 4 to 30 years. HCAP is a cross-sectional random sample of individuals in HRS who were 65 years or older in 2016. Of 9972 age-eligible HRS participants, 4425 were randomly selected for HCAP, and 3496 completed a comprehensive neuropsychological test battery and informant interview, none of whom were excluded. Dementia and MCI were classified using an algorithm based on standard diagnostic criteria and comparing test performance to a robust normative sample.
Exposures: Groups were stratified by age, sex, education, race, and ethnicity.
Main outcomes and measures: National prevalence estimates using population weights.
Results: The mean (SD) age of the study population sample (N = 3496) was 76.4 (7.6) years, and 2095 participants (60%) were female. There were 551 participants who self-identified as Black and not Hispanic (16%), 382 who self-identified as Hispanic regardless of race (16%), 2483 who self-identified as White and not Hispanic (71%), and 80 who self-identified as another race (2%), including American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander, or another self-described race. A total of 393 individuals (10%; 95% CI, 9-11) were classified as having dementia and 804 (22%; 95% CI, 20-24) as having MCI. Every 5-year increase in age was associated with higher risk of dementia (weighted odds ratio [OR], 1.95 per 5-year age difference; 95%, CI, 1.77-2.14) and MCI (OR, 1.17 per 5-year age difference, 95% CI, 1.09-1.26). Each additional year of education was associated with a decrease in risk of dementia (OR, 0.93 per year of school, 95% CI, 0.89-0.97) and MCI (OR, 0.94, 95% CI, 0.91-0.97). Dementia was more common among non-Hispanic Black individuals (OR, 1.81; 95% CI, 1.20-2.75) and MCI in Hispanic individuals (OR, 1.42; 95% CI, 1.03-1.96) compared with non-Hispanic White individuals. Other group comparisons by race and ethnicity were not possible owing to small numbers. No differences in prevalence were found between female individuals and male individuals.
Conclusions and relevance: Using a comprehensive neuropsychological test battery and large sample, the national prevalence of dementia and MCI in 2016 found in this cross-sectional study was similar to that of other US-based studies, indicating a disproportionate burden of dementia and MCI among older Black and Hispanic adults and those with lower education.
Conflict of interest statement
Figures
References
-
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging–Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270-279. doi: 10.1016/j.jalz.2011.03.008 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
