Aortic Arch Variants and Anomalies: Embryology, Imaging Findings, and Clinical Considerations
- PMID: 36280266
- PMCID: PMC9592245
- DOI: 10.4250/jcvi.2022.0058
Aortic Arch Variants and Anomalies: Embryology, Imaging Findings, and Clinical Considerations
Abstract
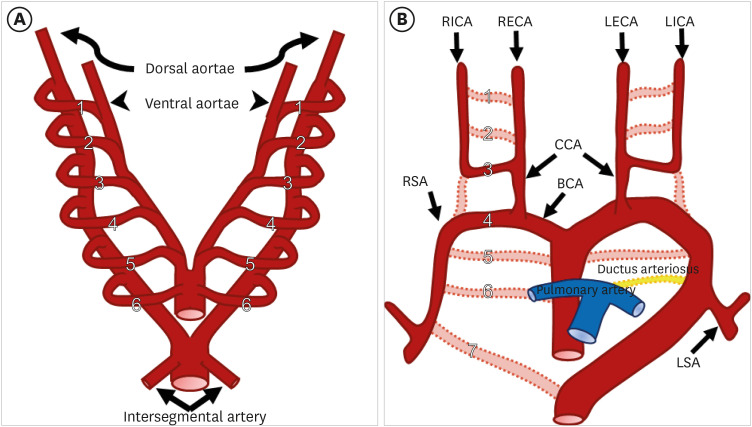
There is a wide spectrum of congenital anomalies or variations of the aortic arch, ranging from non-symptomatic variations that are mostly detected incidentally to clinically symptomatic variations that cause severe respiratory distress or esophageal compression. Some of these may be accompanied by other congenital heart diseases or chromosomal anomalies. The widespread use of multidetector computed tomography (CT) in clinical practice has resulted in incidental detection of several variations of the aortic arch in adults. Thus, radiologists and clinicians should be aware of the classification of aortic arch anomalies and carefully look for imaging features associated with a high risk of clinical symptoms. Understanding the embryological development of the aortic arch aids in the classification of various subtypes of aortic arch anomalies and variants. For accurate diagnosis and precise evaluation of aortic arch anomalies, cross-sectional imaging modalities, such as multidetector CT or magnetic resonance imaging, play an important role by providing three-dimensional reconstructed images. In this review, we describe the embryological development of the thoracic aorta and discuss variations and anomalies of the aortic arch along with their clinical implications.
Keywords: Aorta; Congenital abnormalities; Multidetector computed tomography; Technology.
Copyright © 2022 Korean Society of Echocardiography.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
Congenital Variants and Anomalies of the Aortic Arch.Radiographics. 2017 Jan-Feb;37(1):32-51. doi: 10.1148/rg.2017160033. Epub 2016 Nov 18. Radiographics. 2017. PMID: 27860551 Review.
-
Anomalies of the aortic arch in dogs: evaluation with the use of multidetector computed tomography angiography and proposal of an extended classification scheme.BMC Vet Res. 2021 Dec 16;17(1):387. doi: 10.1186/s12917-021-03101-7. BMC Vet Res. 2021. PMID: 34915887 Free PMC article.
-
Aortic arch anomalies, embryology and their relevance in neuro-interventional surgery and stroke: A review.Interv Neuroradiol. 2022 Aug;28(4):489-498. doi: 10.1177/15910199211039924. Epub 2021 Sep 13. Interv Neuroradiol. 2022. PMID: 34516323 Free PMC article. Review.
-
Congenital thoracic arterial anomalies in adults: a CT overview.Diagn Interv Radiol. 2011 Dec;17(4):352-62. doi: 10.4261/1305-3825.DIR.4645-11.1. Epub 2011 Oct 6. Diagn Interv Radiol. 2011. PMID: 21975665
-
Congenital anomalies of the aortic arch: evaluation with the use of multidetector computed tomography.Korean J Radiol. 2009 Mar-Apr;10(2):176-84. doi: 10.3348/kjr.2009.10.2.176. Epub 2009 Mar 3. Korean J Radiol. 2009. PMID: 19270864 Free PMC article. Review.
Cited by
-
A comparative analysis of CT angiography and echocardiography in the evaluation of chest findings in patients with interrupted aortic arch.Front Radiol. 2025 Jun 26;5:1616112. doi: 10.3389/fradi.2025.1616112. eCollection 2025. Front Radiol. 2025. PMID: 40642309 Free PMC article.
-
Medical-Surgical Implications of Branching Variation of Human Aortic Arch Known as Bovine Aortic Arch (BAA).J Pers Med. 2024 Jun 24;14(7):678. doi: 10.3390/jpm14070678. J Pers Med. 2024. PMID: 39063932 Free PMC article. Review.
-
CT Angiography for Aortic Arch Anomalies: Prevalence, Diagnostic Efficacy, and Illustrative Findings.Diagnostics (Basel). 2024 Aug 24;14(17):1851. doi: 10.3390/diagnostics14171851. Diagnostics (Basel). 2024. PMID: 39272636 Free PMC article.
-
Thoracic Aorta: Anatomy and Pathology.Diagnostics (Basel). 2023 Jun 25;13(13):2166. doi: 10.3390/diagnostics13132166. Diagnostics (Basel). 2023. PMID: 37443560 Free PMC article. Review.
-
A rare variation of five major vessels arising from the aortic arch with an absence of brachiocephalic trunk.Surg Radiol Anat. 2025 Jun 19;47(1):161. doi: 10.1007/s00276-025-03674-0. Surg Radiol Anat. 2025. PMID: 40537711 Free PMC article.
References
-
- Goldmuntz E. The epidemiology and genetics of congenital heart disease. Clin Perinatol. 2001;28:1–10. - PubMed
-
- Kocis KC, Midgley FM, Ruckman RN. Aortic arch complex anomalies: 20-year experience with symptoms, diagnosis, associated cardiac defects, and surgical repair. Pediatr Cardiol. 1997;18:127–132. - PubMed
-
- Jakanani GC, Adair W. Frequency of variations in aortic arch anatomy depicted on multidetector CT. Clin Radiol. 2010;65:481–487. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources