

Astrocytes in the initiation and progression of epilepsy
- PMID: 36280704
- PMCID: PMC10368155
- DOI: 10.1038/s41582-022-00727-5
Astrocytes in the initiation and progression of epilepsy
Abstract
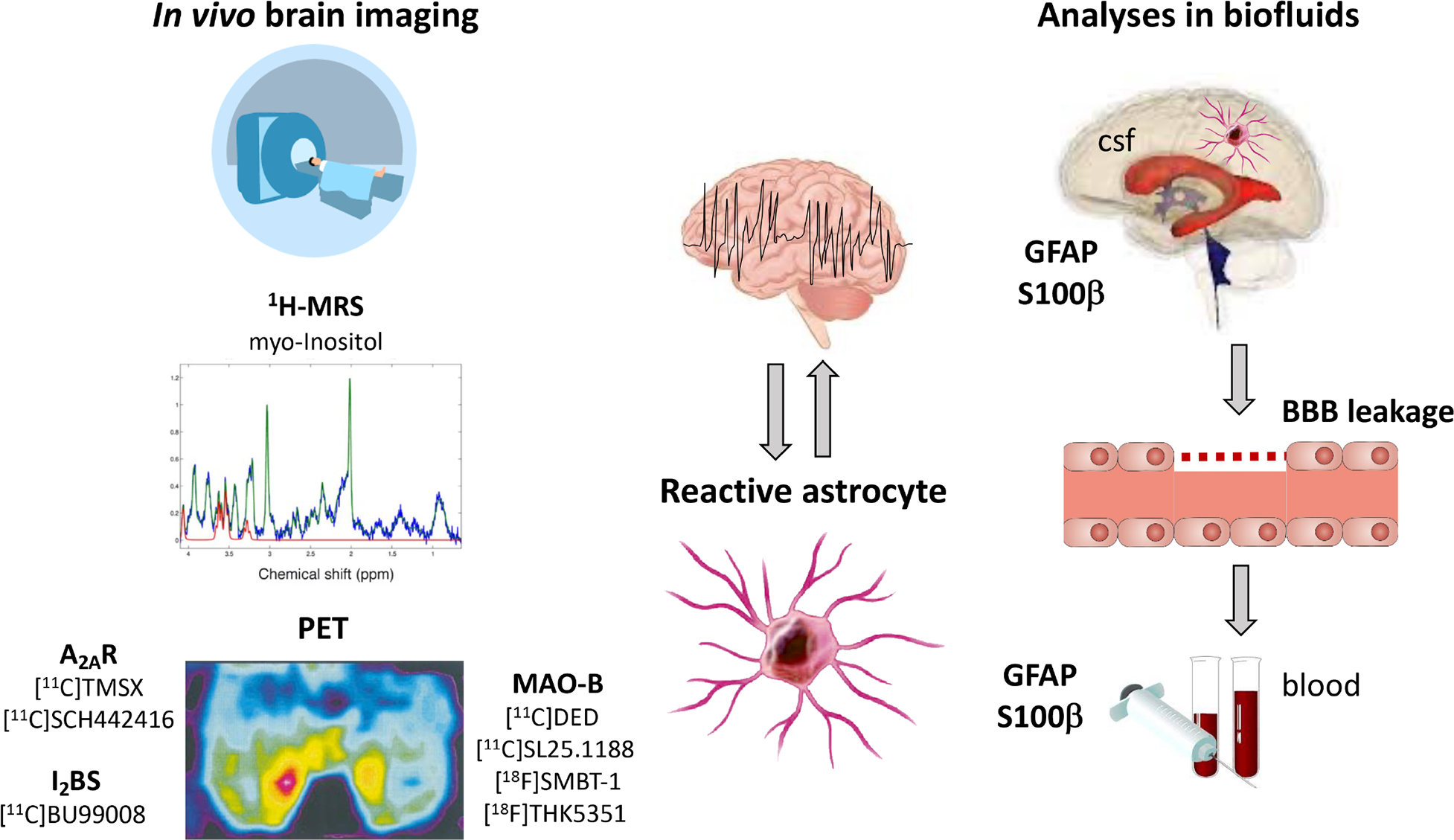
Epilepsy affects ~65 million people worldwide. First-line treatment options include >20 antiseizure medications, but seizure control is not achieved in approximately one-third of patients. Antiseizure medications act primarily on neurons and can provide symptomatic control of seizures, but do not alter the onset and progression of epilepsy and can cause serious adverse effects. Therefore, medications with new cellular and molecular targets and mechanisms of action are needed. Accumulating evidence indicates that astrocytes are crucial to the pathophysiological mechanisms of epilepsy, raising the possibility that these cells could be novel therapeutic targets. In this Review, we discuss how dysregulation of key astrocyte functions - gliotransmission, cell metabolism and immune function - contribute to the development and progression of hyperexcitability in epilepsy. We consider strategies to mitigate astrocyte dysfunction in each of these areas, and provide an overview of how astrocyte activation states can be monitored in vivo not only to assess their contribution to disease but also to identify markers of disease processes and treatment effects. Improved understanding of the roles of astrocytes in epilepsy has the potential to lead to novel therapies to prevent the initiation and progression of epilepsy.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests
The authors declare no competing interests
Figures



References
-
-
Khakh BS & Deneen B The Emerging Nature of Astrocyte Diversity. Annu Rev Neurosci 42, 187–207 (2019).
*This review emphasizes that astrocytes represent a diverse population of cells and that they display brain area- and disease-specific properties and functions. Knowledge gaps are identified that need to be addressed in order to elucidate astrocyte diversity and its physiological relevance in the CNS.
-
-
- Araque A, Parpura V, Sanzgiri RP & Haydon PG Tripartite synapses: glia, the unacknowledged partner. Trends Neurosci 22, 208–215 (1999). - PubMed
-
- Devinsky O, Vezzani A, Najjar S, De Lanerolle NC & Rogawski MA Glia and epilepsy: excitability and inflammation. Trends Neurosci 36, 174–84 (2013). - PubMed
