

CODA: quantitative 3D reconstruction of large tissues at cellular resolution
- PMID: 36280719
- PMCID: PMC10500590
- DOI: 10.1038/s41592-022-01650-9
CODA: quantitative 3D reconstruction of large tissues at cellular resolution
Abstract
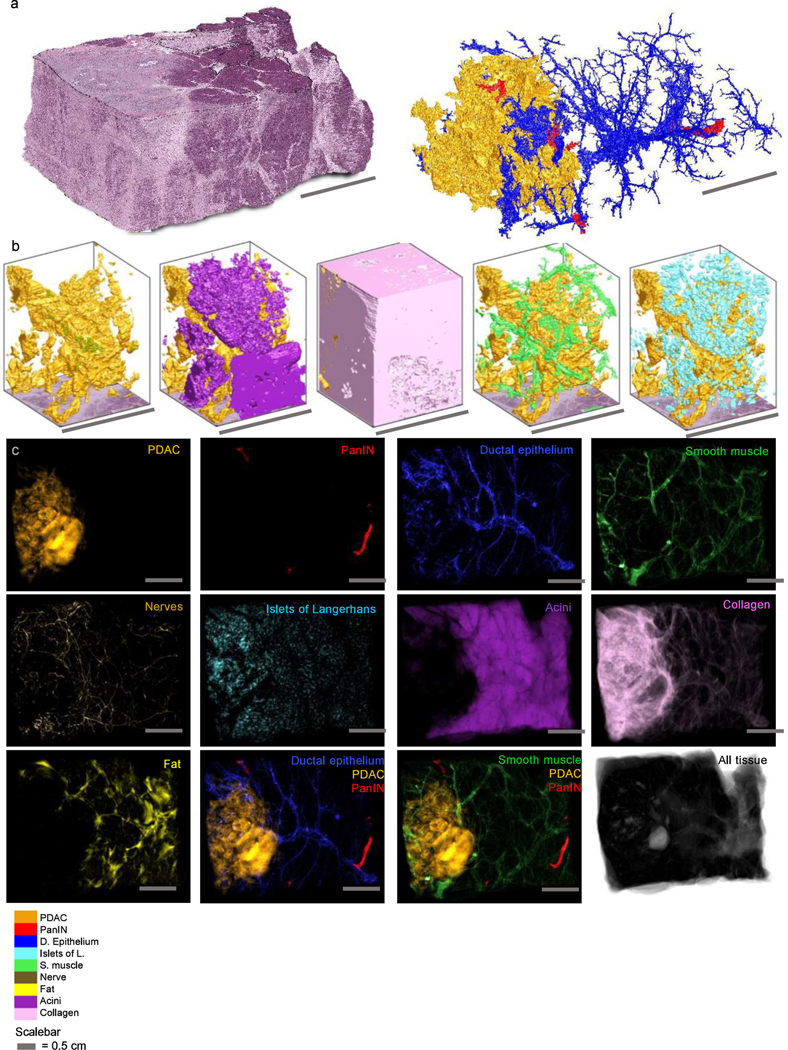
A central challenge in biology is obtaining high-content, high-resolution information while analyzing tissue samples at volumes relevant to disease progression. We address this here with CODA, a method to reconstruct exceptionally large (up to multicentimeter cubed) tissues at subcellular resolution using serially sectioned hematoxylin and eosin-stained tissue sections. Here we demonstrate CODA's ability to reconstruct three-dimensional (3D) distinct microanatomical structures in pancreas, skin, lung and liver tissues. CODA allows creation of readily quantifiable tissue volumes amenable to biological research. As a testbed, we assess the microanatomy of the human pancreas during tumorigenesis within the branching pancreatic ductal system, labeling ten distinct structures to examine heterogeneity and structural transformation during neoplastic progression. We show that pancreatic precancerous lesions develop into distinct 3D morphological phenotypes and that pancreatic cancer tends to spread far from the bulk tumor along collagen fibers that are highly aligned to the 3D curves of ductal, lobular, vascular and neural structures. Thus, CODA establishes a means to transform broadly the structural study of human diseases through exploration of exhaustively labeled 3D microarchitecture.
© 2022. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Figures













References
-
- Liebig C, Ayala G, Wilks JA, Berger DH & Albo D. Perineural invasion in cancer. Cancer 115, 3379–3391 (2009). - PubMed
-
- Siegel RL, Miller KD, Fuchs HE & Jemal A. Cancer Statistics, 2021. CA. Cancer J. Clin. 71, 7–33 (2021). - PubMed
-
- Michaud DS et al. Physical Activity, Obesity, Height, and the Risk of Pancreatic Cancer. JAMA 286, 921–929 (2001). - PubMed
-
- Hruban RH et al. Why is pancreatic cancer so deadly? The pathologist’s view. J. Pathol. 248, 131–141 (2019). - PubMed
Online Methods References:
-
- Graham S. et al. Hover-Net: Simultaneous segmentation and classification of nuclei in multi-tissue histology images. Med. Image Anal. 58, 101563 (2019). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
