

Hyperlipidemia and mortality in patients on peritoneal dialysis
- PMID: 36280801
- PMCID: PMC9590170
- DOI: 10.1186/s12882-022-02970-w
Hyperlipidemia and mortality in patients on peritoneal dialysis
Abstract
Background: New lipid-lowering therapy at the start of dialysis and measurement of lipid parameters over the follow-up period is not recommended in dialysis patients, which seems unappropriated in clinical practice. We aimed to examine the effect of hyperlipidemia on mortality in patients undergoing continuous ambulatory peritoneal dialysis (CAPD).
Methods: A retrospective cohort study was performed, including 2939 incident CAPD patients from five dialysis facilities between January 1, 2005, and December 31, 2018. The primary outcome was all-cause mortality. The association between hyperlipidemia at the start of CAPD and all-cause mortality was evaluated using Cox proportional hazards regression.
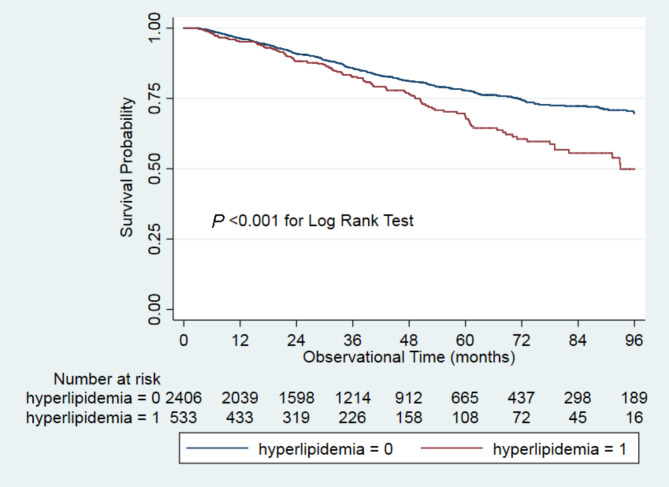
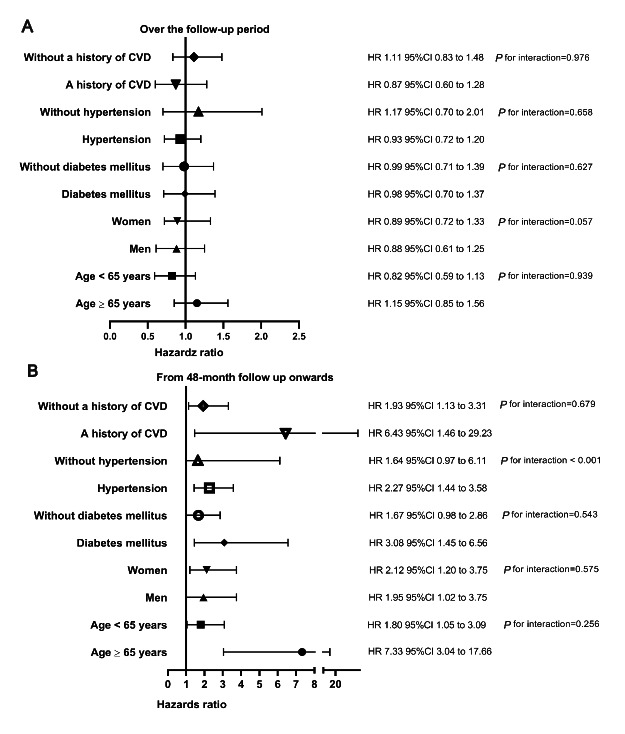
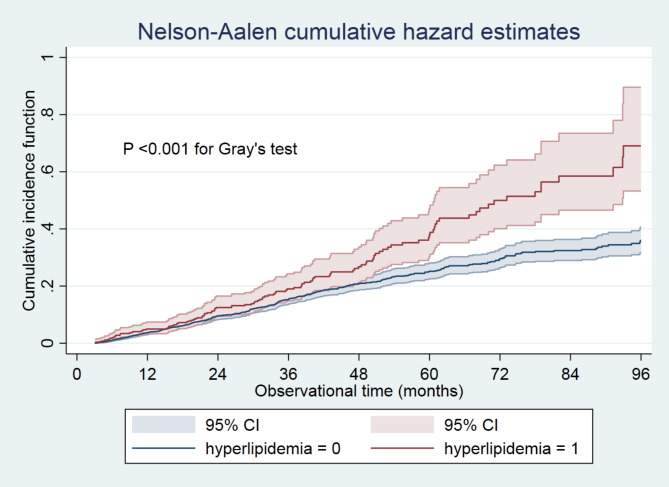
Results: Of 2939 with a median age of 50.0 (interquartile range, 39.0-61.0), 1697 (57.7%) were men, 533 (18.1%) had hyperlipidemia, 549 (18.7%) had diabetes mellitus, 1915 (65.2%) had hypertension, and 410 (14.0%) had a history of CVD. During the median follow-up period of 35.1 months, 519 (17.7%) died, including 402 (16.7%, 47.4/1000 patient-years) in the non-hyperlipidemia group and 117 (22.0%, 71.1/1000 patient-years) in the hyperlipidemia group. Over the overall follow-up period, patients with hyperlipidemia had an equally high risk of all-cause mortality throughout follow-up as those without hyperlipidemia ([HR] 1.04, 95% confidence interval [CI] 0.83 to 1.31). However, from the 48-month follow-up onwards, hyperlipidemia was associated with a 2.26 (95% CI 1.49 to 3.43)-time higher risk of all-cause mortality than non-hyperlipidemia. Hypertension modified the association between hyperlipidemia and all-cause mortality (P for interaction < 0.001). A significantly increased risk of all-cause mortality was observed among patients with hypertension (HR 2.27, 95%CI 1.44-3.58).
Conclusion: Among CAPD patients, hyperlipidemia at the beginning of CAPD was associated with a high risk of long-term mortality. Hypertension may mediate the association. Our findings suggested that long-term lipid-lowering treatment should be used in those patients with hyperlipidemia.
Keywords: Hyperlipidemia; Hypertension; Mortality; Peritoneal dialysis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet. 2011;377:2181–92. doi: 10.1016/S0140-6736(11)60739-3. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
