

Association of the medical therapy with beta-blockers or inhibitors of renin-angiotensin system with clinical outcomes in patients with mildly reduced left ventricular ejection fraction after acute myocardial infarction
- PMID: 36281078
- PMCID: PMC9592534
- DOI: 10.1097/MD.0000000000030846
Association of the medical therapy with beta-blockers or inhibitors of renin-angiotensin system with clinical outcomes in patients with mildly reduced left ventricular ejection fraction after acute myocardial infarction
Abstract
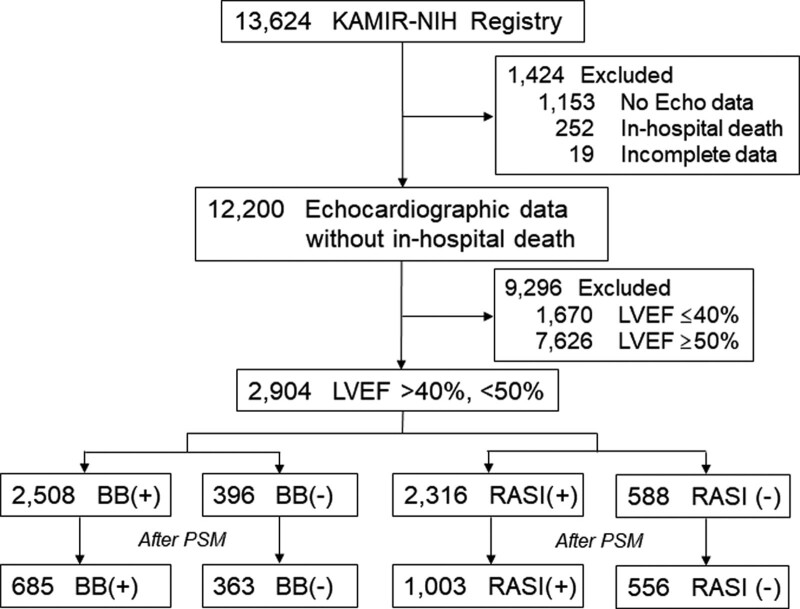
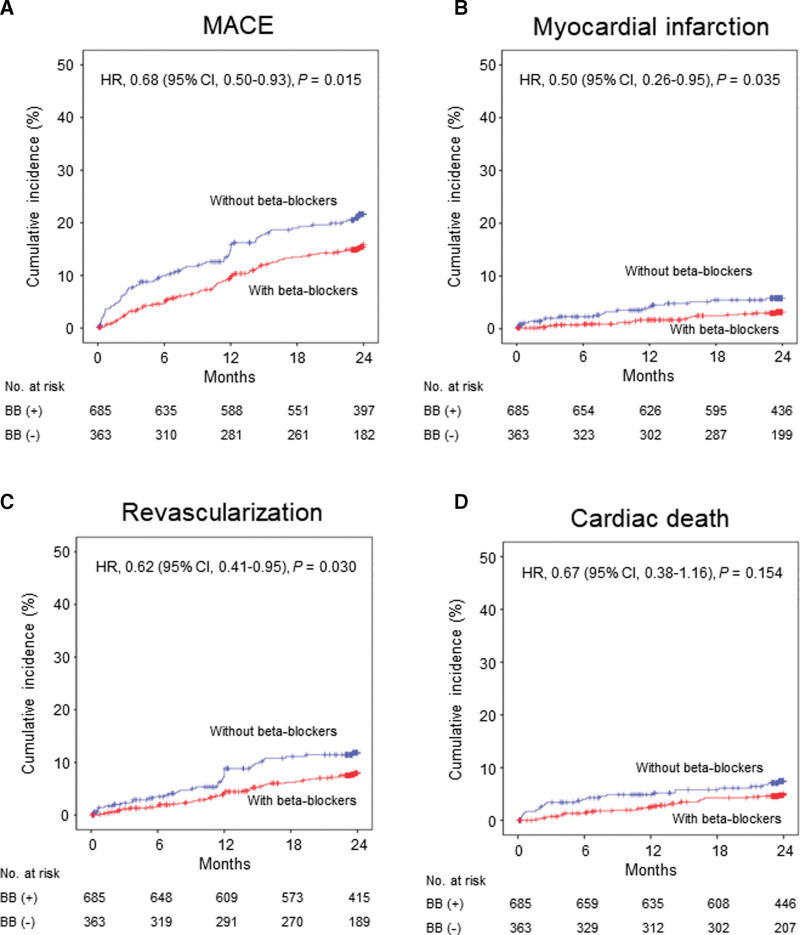
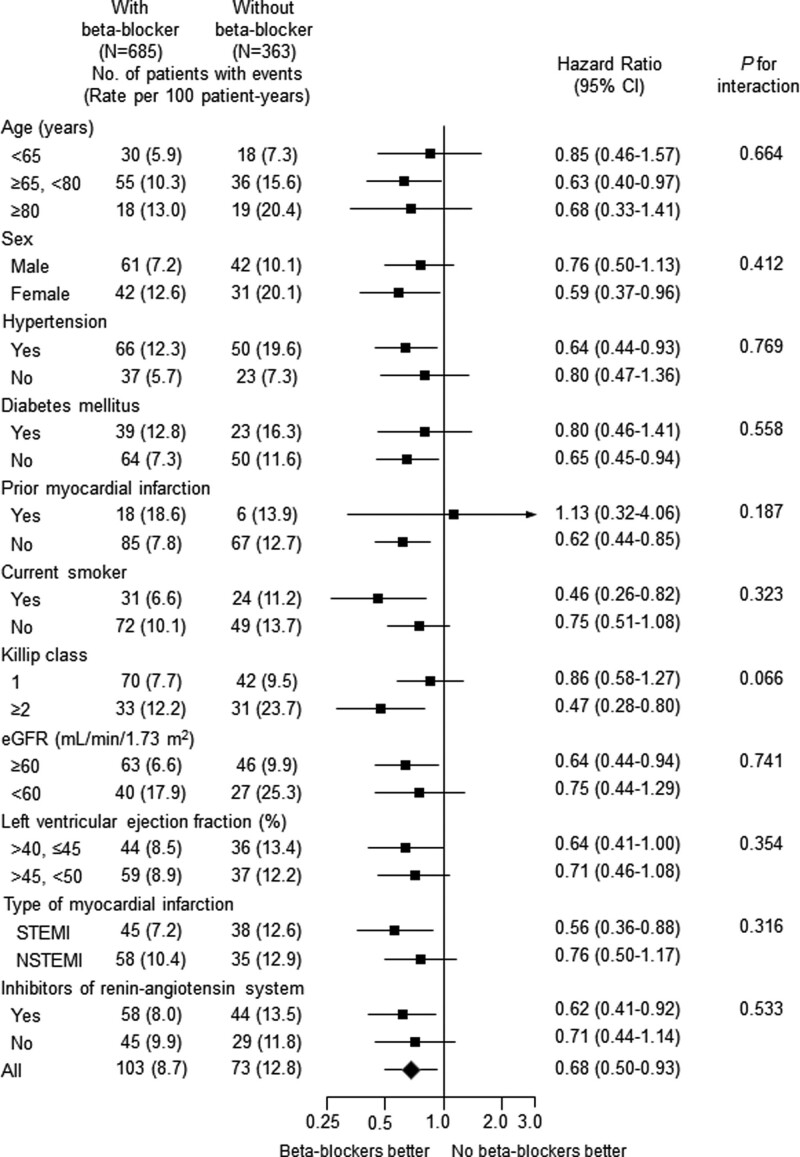
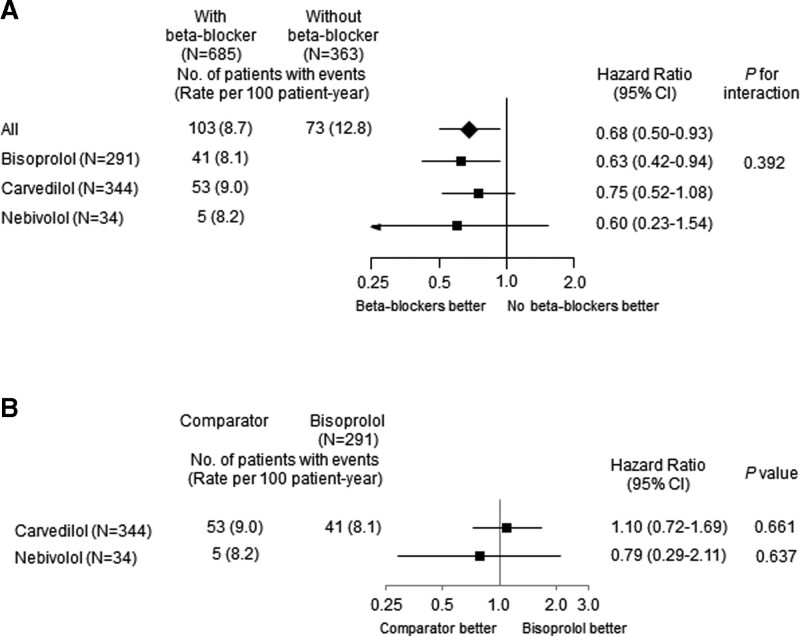
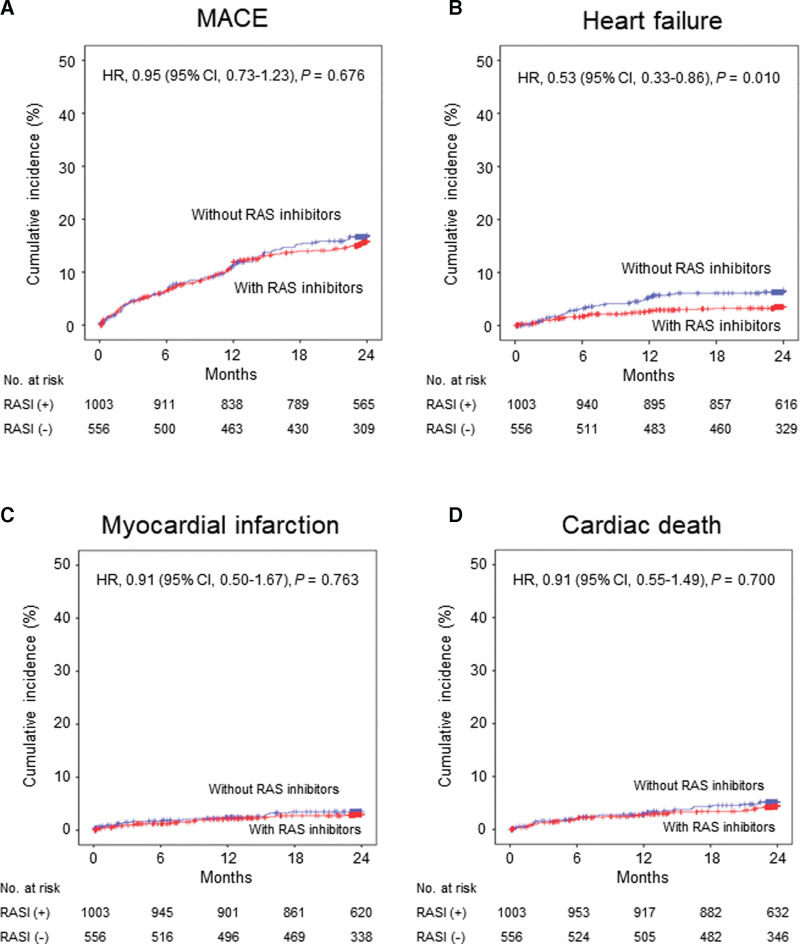
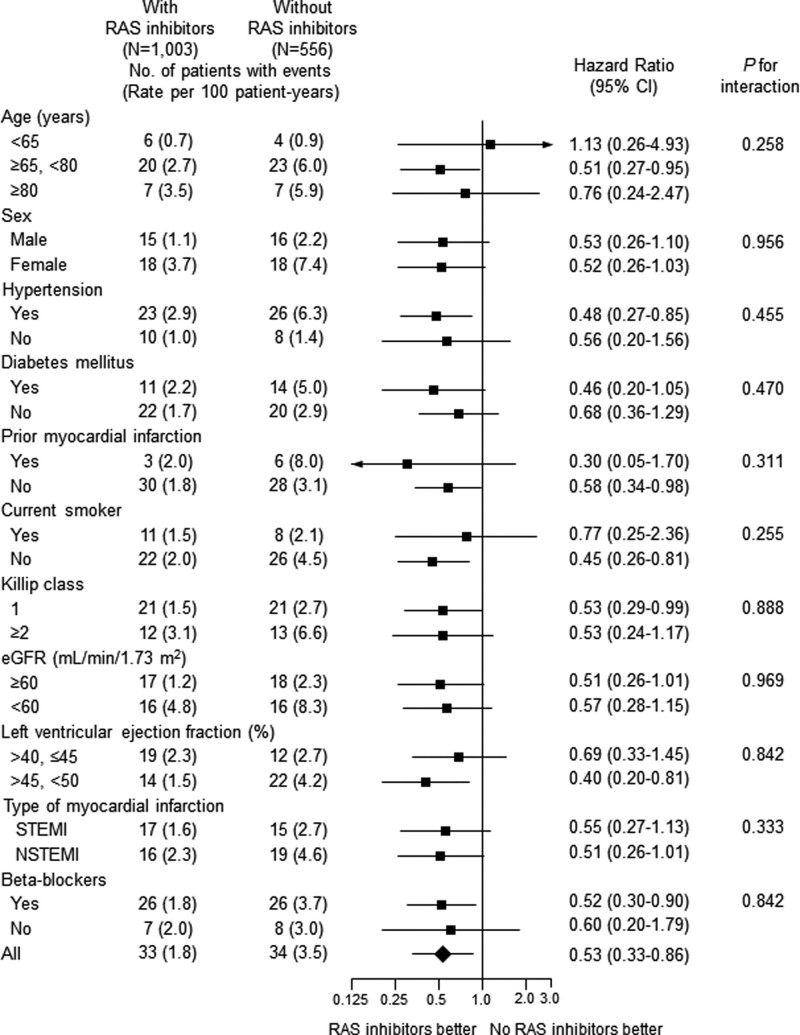
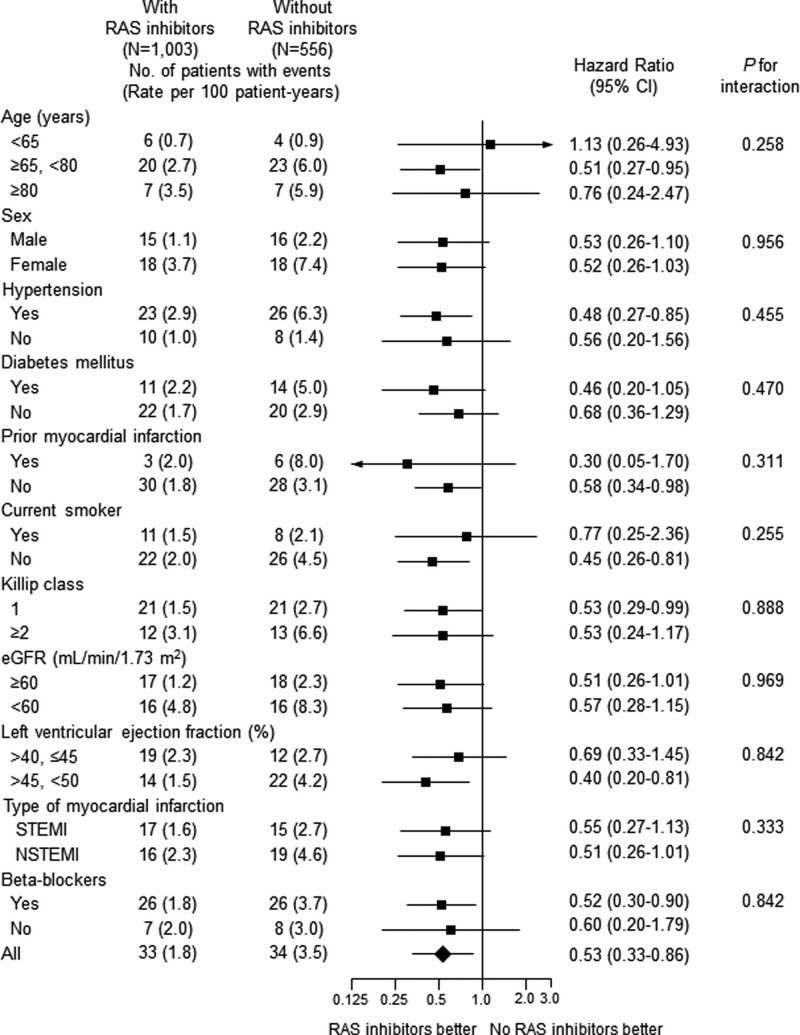
In the era of the initial optimal interventional and medical therapy for acute myocardial infarction (AMI), a number of patients with mildly reduced left ventricular ejection fraction (EF) (41%-49%) have been increasing. This observational study aimed to investigate the association between the medical therapy with oral beta-blockers or inhibitors of renin-angiotensin system (RAS) and 2-year clinical outcomes in patients with mildly reduced EF after AMI. Among patients enrolled in the Korea Acute Myocardial Infarction Registry-National Institute of Health, propensity-score matched patients who survived the initial attack and had mildly reduced EF were selected according to beta-blocker or RAS inhibitor therapy at discharge. Beta-blocker therapy at discharge was associated with lower 2-year major adverse cardiac events which was a composite of cardiac death, myocardial infarction, revascularization and re-hospitalization due to heart failure (8.7 vs 12.8/100 patient-years; hazard ratio [HR] 0.68; 95% confidence interval [CI] 0.50-0.93; P = .015), and no significant interaction between EF ≤ 45% and > 45% was observed (Pinteraction = 0.354). This association was mainly driven by lower myocardial infarction in patients with beta-blockers (HR 0.50; 95% CI 0.26-0.95; P = .035). Inhibitors of RAS at discharge were associated with lower re-hospitalization due to heart failure (1.8 vs 3.5/100 patient-years; HR 0.53; 95% CI 0.33-0.86; P = .010) without a significant interaction between EF ≤ 45% and > 45% (Pinteraction = 0.333). In patients with mildly reduced EF after AMI, the medical therapy with beta-blockers or RAS inhibitors at discharge was associated with better 2-year clinical outcomes.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, et al. . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–200. - PubMed
-
- McDonagh TA, Metra M, Adamo M, et al. . 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42:3599–726. - PubMed
-
- The CAPRICON Investigators. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet. 2001;357:1385–90. - PubMed
-
- Flather MD, Yusuf S, Køber L, et al. . Long-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: a systematic overview of data from individual patients. Lancet. 2000;355:1575–81. - PubMed
-
- Pfeffer MA, McMurray JJ, Velazquez EJ, et al. . Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both. N Engl J Med. 2003;349:1893–906. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
