Documenting the Recovery of Vascular Services in European Centres Following the Initial COVID-19 Pandemic Peak: Results from a Multicentre Collaborative Study
- PMID: 36281225
- PMCID: PMC9581639
- DOI: 10.1016/j.ejvsvf.2022.10.002
Documenting the Recovery of Vascular Services in European Centres Following the Initial COVID-19 Pandemic Peak: Results from a Multicentre Collaborative Study
Abstract
Objective: To document the recovery of vascular services in Europe following the first COVID-19 pandemic peak.
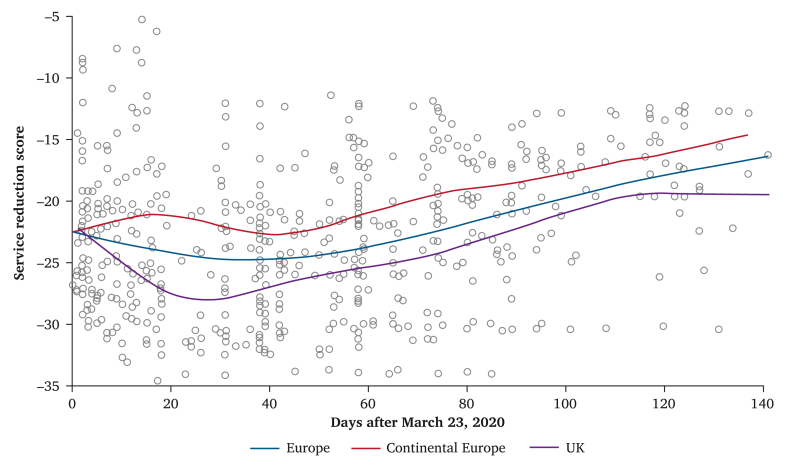
Methods: An online structured vascular service survey with repeated data entry between 23 March and 9 August 2020 was carried out. Unit level data were collected using repeated questionnaires addressing modifications to vascular services during the first peak (March - May 2020, "period 1"), and then again between May and June ("period 2") and June and July 2020 ("period 3"). The duration of each period was similar. From 2 June, as reductions in cases began to be reported, centres were first asked if they were in a region still affected by rising cases, or if they had passed the peak of the first wave. These centres were asked additional questions about adaptations made to their standard pathways to permit elective surgery to resume.
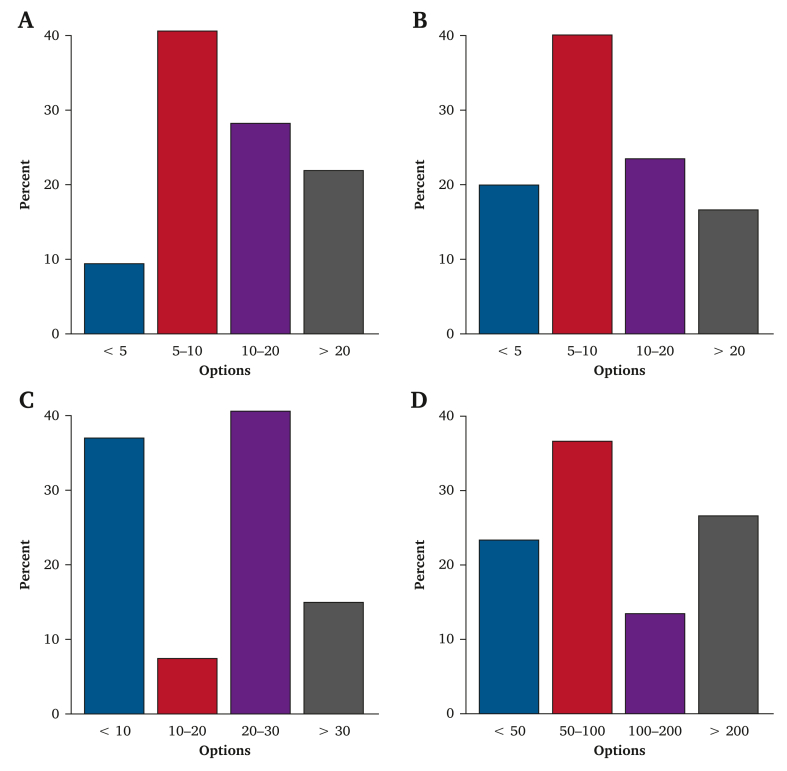
Results: The impact of the pandemic continued to be felt well after countries' first peak was thought to have passed in 2020. Aneurysm screening had not returned to normal in 21.7% of centres. Carotid surgery was still offered on a case by case basis in 33.8% of centres, and only 52.9% of centres had returned to their normal aneurysm threshold for surgery. Half of centres (49.4%) believed their management of lower limb ischaemia continued to be negatively affected by the pandemic. Reduced operating theatre capacity continued in 45.5% of centres. Twenty per cent of responding centres documented a backlog of at least 20 aortic repairs. At least one negative swab and 14 days of isolation were the most common strategies used for permitting safe elective surgery to recommence.
Conclusion: Centres reported a broad return of services approaching pre-pandemic "normal" by July 2020. Many introduced protocols to manage peri-operative COVID-19 risk. Backlogs in cases were reported for all major vascular surgeries.
Keywords: AAA; COVID-19; PAD; Survey; Vascular surgery.
© 2022 The Author(s).
Figures