

Precuneus magnetic stimulation for Alzheimer's disease: a randomized, sham-controlled trial
- PMID: 36281767
- PMCID: PMC9679166
- DOI: 10.1093/brain/awac285
Precuneus magnetic stimulation for Alzheimer's disease: a randomized, sham-controlled trial
Abstract
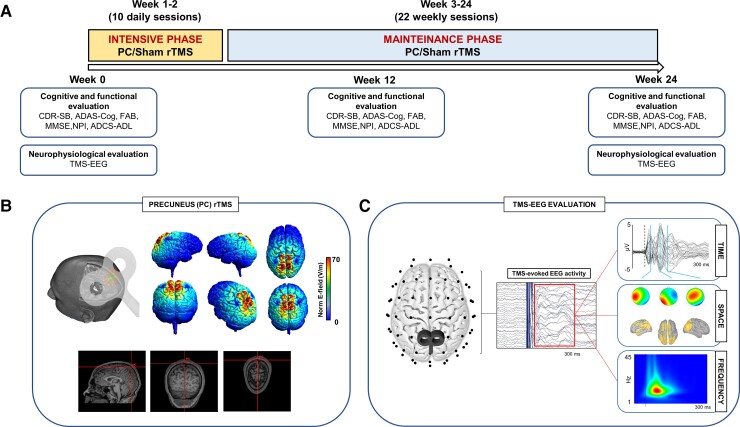
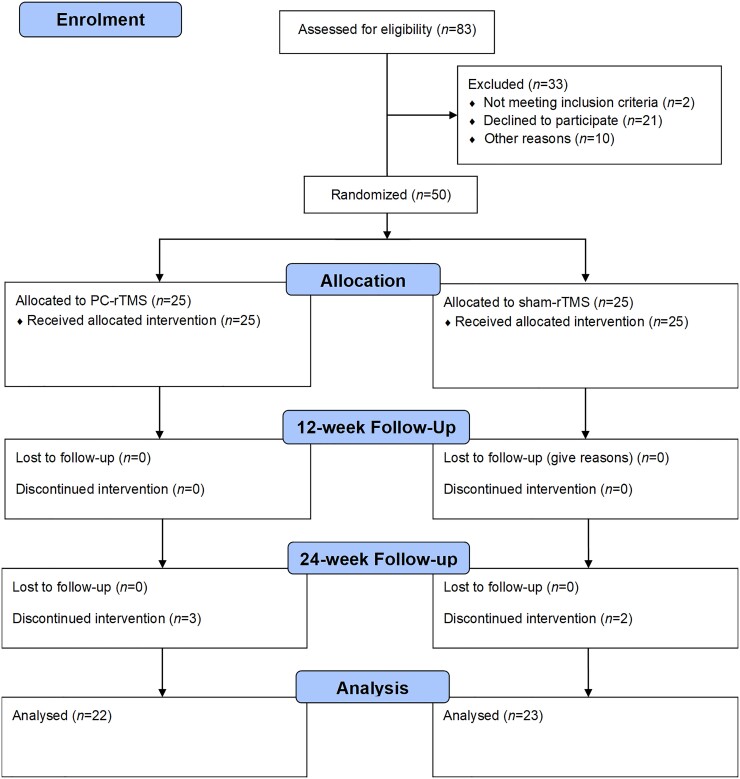
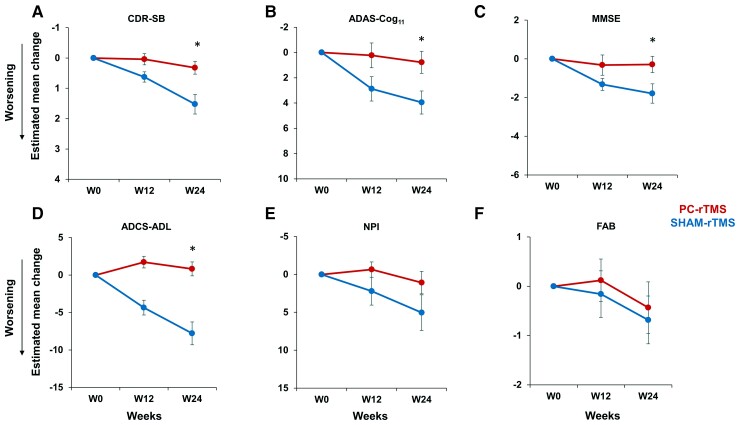
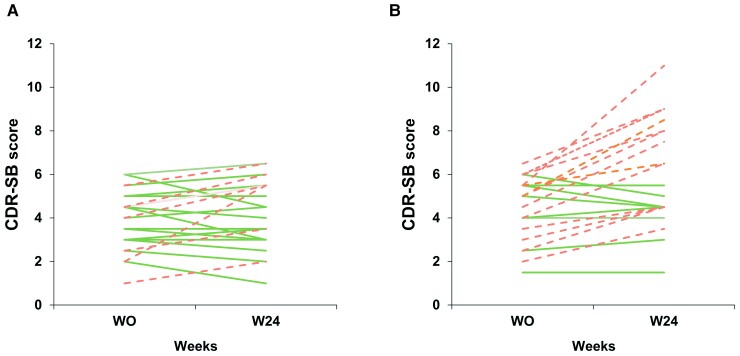
Repetitive transcranial magnetic stimulation (rTMS) is emerging as a non-invasive therapeutic strategy in the battle against Alzheimer's disease. Alzheimer's disease patients primarily show alterations of the default mode network for which the precuneus is a key node. Here, we hypothesized that targeting the precuneus with TMS represents a promising strategy to slow down cognitive and functional decline in Alzheimer's disease patients. We performed a randomized, double-blind, sham-controlled, phase 2, 24-week trial to determine the safety and efficacy of precuneus stimulation in patients with mild-to-moderate Alzheimer's disease. Fifty Alzheimer's disease patients were randomly assigned in a 1:1 ratio to either receive precuneus or sham rTMS (mean age 73.7 years; 52% female). The trial included a 24-week treatment, with a 2-week intensive course in which rTMS (or sham) was applied daily five times per week, followed by a 22-week maintenance phase in which stimulation was applied once weekly. The Clinical Dementia Rating Scale-Sum of Boxes was selected as the primary outcome measure, in which post-treatment scores were compared to baseline. Secondary outcomes included score changes in the Alzheimer's Disease Assessment Scale-Cognitive Subscale, Mini-Mental State Examination and Alzheimer's Disease Cooperative Study-Activities of Daily Living scale. Moreover, single-pulse TMS in combination with EEG was used to assess neurophysiological changes in precuneus cortical excitability and oscillatory activity. Our findings show that patients that received precuneus repetitive magnetic stimulation presented a stable performance of the Clinical Dementia Rating Scale-Sum of Boxes score, whereas patients treated with sham showed a worsening of their score. Compared with the sham stimulation, patients in the precuneus stimulation group also showed also significantly better performances for the secondary outcome measures, including the Alzheimer's Disease Assessment Scale-Cognitive Subscale, Mini-Mental State Examination and Alzheimer's Disease Cooperative Study-Activities of Daily Living scale. Neurophysiological results showed that precuneus cortical excitability remained unchanged after 24 weeks in the precuneus stimulation group, whereas it was significantly reduced in the sham group. Finally, we found an enhancement of local gamma oscillations in the group treated with precuneus stimulation but not in patients treated with sham. We conclude that 24 weeks of precuneus rTMS may slow down cognitive and functional decline in Alzheimer's disease. Repetitive TMS targeting the default mode network could represent a novel therapeutic approach in Alzheimer's disease patients.
Keywords: Alzheimer’s disease; default mode network; plasticity; precuneus; transcranial magnetic stimulation.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures

Comment in
-
Repetitive TMS applied to the precuneus stabilizes cognitive status in Alzheimer's disease.Brain. 2022 Nov 21;145(11):3730-3732. doi: 10.1093/brain/awac322. Brain. 2022. PMID: 36412517 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
