

Handling of the Covid-19 Pandemic and Its Effects on Bariatric Surgical Practice: Analysis of GENEVA Study Database
- PMID: 36282429
- PMCID: PMC9592878
- DOI: 10.1007/s11695-022-06267-7
Handling of the Covid-19 Pandemic and Its Effects on Bariatric Surgical Practice: Analysis of GENEVA Study Database
Abstract
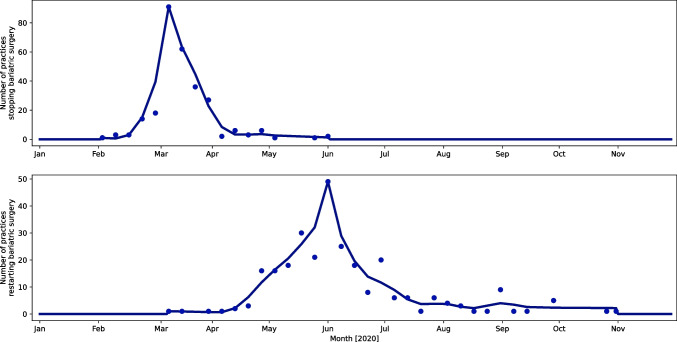
Background: The coronavirus disease 2019 (COVID-19) pandemic led to a worldwide suspension of bariatric and metabolic surgery (BMS) services. The current study analyses data on patterns of service delivery, recovery of practices, and protective measures taken during the COVID-19 pandemic by bariatric teams.
Materials and methods: The current study is a subset analysis of the GENEVA study which was an international cohort study between 01/05/2020 and 31/10/2020. Data were specifically analysed regarding the timing of BMS suspension, patterns of service recovery, and precautionary measures deployed.
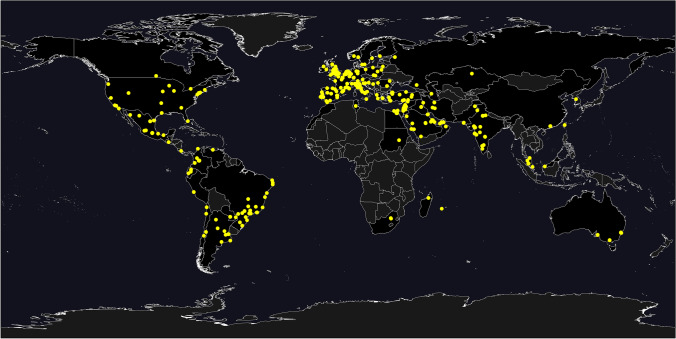
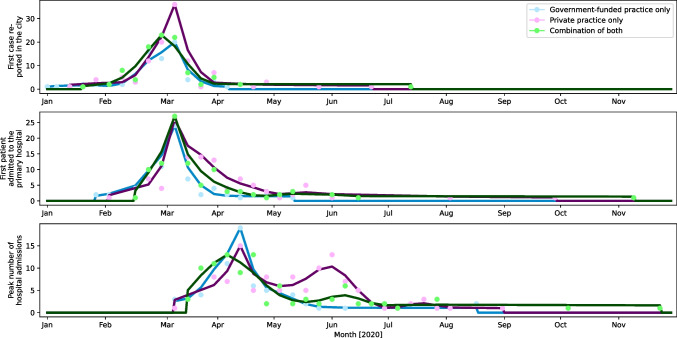
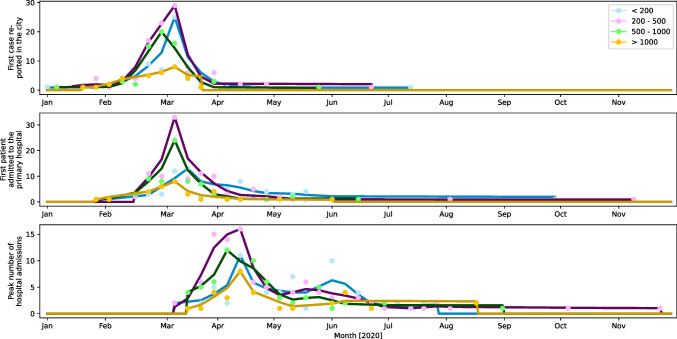
Results: A total of 527 surgeons from 439 hospitals in 64 countries submitted data regarding their practices and handling of the pandemic. Smaller hospitals (with less than 200 beds) were able to restart BMS programmes more rapidly (time to BMS restart 60.8 ± 38.9 days) than larger institutions (over 2000 beds) (81.3 ± 30.5 days) (p = 0.032). There was a significant difference in the time interval between cessation/reduction and restart of bariatric services between government-funded practices (97.1 ± 76.2 days), combination practices (84.4 ± 47.9 days), and private practices (58.5 ± 38.3 days) (p < 0.001). Precautionary measures adopted included patient segregation, utilisation of personal protective equipment, and preoperative testing. Following service recovery, 40% of the surgeons operated with a reduced capacity. Twenty-two percent gave priority to long waiters, 15.4% gave priority to uncontrolled diabetics, and 7.6% prioritised patients requiring organ transplantation.
Conclusion: This study provides global, real-world data regarding the recovery of BMS services following the COVID-19 pandemic.
Keywords: Bariatric surgery; COVID-19; GENEVA; Global health; Pandemic; Public health; SARS-CoV-2.
© 2022. The Author(s).
Conflict of interest statement
A. A. T. reports grants from Novo Nordisk, personal fees from Novo Nordisk, non-financial support from Novo Nordisk, personal fees from Eli Lilly, non-financial support from Eli Lilly, personal fees from Janssen, personal fees from AZ, non-financial support from AZ, non-financial support from Impeto medical, non-financial support from Resmed, non-financial support from Aptiva, personal fees from BI, non-financial support from BI, personal fees from BMS, non-financial support from BMS, personal fees from NAPP, non-financial support from NAPP, personal fees from MSD, non-financial support from MSD, personal fees from Nestle, personal fees from Gilead, grants from Sanofi, and personal fees from Sanofi outside the submitted work. A. A. T. is currently an employee of Novo Nordisk. Novo Nordisk had no role in this project.
K. M. has been paid honoraria by various NHS trusts and Ethicon®, Medtronic®, Gore Inc®, and Olympus® for educational activities related to bariatric surgery.
Other authors have no conflicts of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
