

The Notch1/CD22 signaling axis disrupts Treg function in SARS-CoV-2-associated multisystem inflammatory syndrome in children
- PMID: 36282598
- PMCID: PMC9797337
- DOI: 10.1172/JCI163235
The Notch1/CD22 signaling axis disrupts Treg function in SARS-CoV-2-associated multisystem inflammatory syndrome in children
Abstract
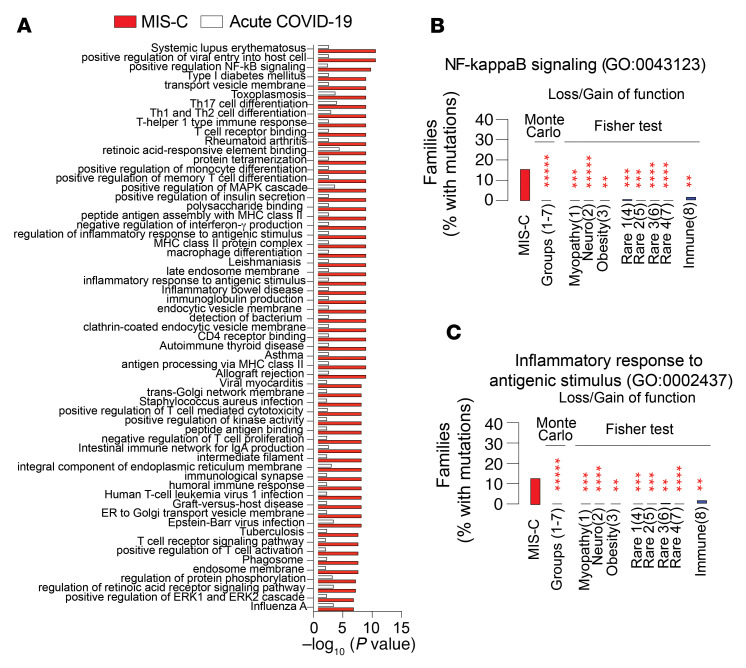
Multisystem inflammatory syndrome in children (MIS-C) evolves in some pediatric patients following acute infection with SARS-CoV-2 by hitherto unknown mechanisms. Whereas acute-COVID-19 severity and outcomes were previously correlated with Notch4 expression on Tregs, here, we show that Tregs in MIS-C were destabilized through a Notch1-dependent mechanism. Genetic analysis revealed that patients with MIS-C had enrichment of rare deleterious variants affecting inflammation and autoimmunity pathways, including dominant-negative mutations in the Notch1 regulators NUMB and NUMBL leading to Notch1 upregulation. Notch1 signaling in Tregs induced CD22, leading to their destabilization in a mTORC1-dependent manner and to the promotion of systemic inflammation. These results identify a Notch1/CD22 signaling axis that disrupts Treg function in MIS-C and point to distinct immune checkpoints controlled by individual Treg Notch receptors that shape the inflammatory outcome in SARS-CoV-2 infection.
Keywords: Adaptive immunity; COVID-19; Immunology; T cells; Tolerance.
Figures








Comment in
-
Notch1 signaling impairs regulatory T cells during multisystem inflammatory syndrome in children.J Clin Invest. 2023 Jan 3;133(1):e166016. doi: 10.1172/JCI166016. J Clin Invest. 2023. PMID: 36594470 Free PMC article.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
