

Adhesive capsulitis and ultrasound diagnosis, an inseparable pair: a novel review
- PMID: 36284048
- PMCID: PMC10247624
- DOI: 10.1007/s40477-022-00725-9
Adhesive capsulitis and ultrasound diagnosis, an inseparable pair: a novel review
Abstract
Purpose: Adhesive Capsulitis (AC) is a musculoskeletal disorder initially described by Codman in 1934. The disease is characterized by pain-limited restriction in active and passive glenohumeral range of motion (ROM) despite the lack of a structural deficit. In the last decades, arthroscopy and magnetic resonance imaging (MRI) has been the only diagnostic tools able to highlight the characteristic alterations of the glenohumeral capsular-ligament apparatus in AC; nevertheless, both arthroscopy and MRI are burdened by intrinsic limitations. The aim of this narrative review is to summarize the most significant evidence supporting the use of ultrasound (US) for the diagnosis of AC.
Methods: We extensively searched via PubMed library the terms "frozen-shoulder" and "adhesive capsulitis" each combined with "ultrasound".
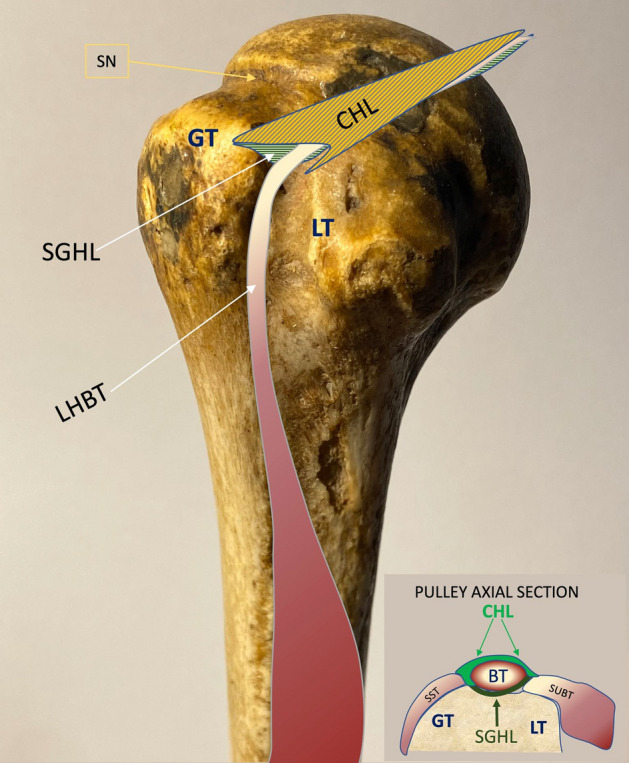
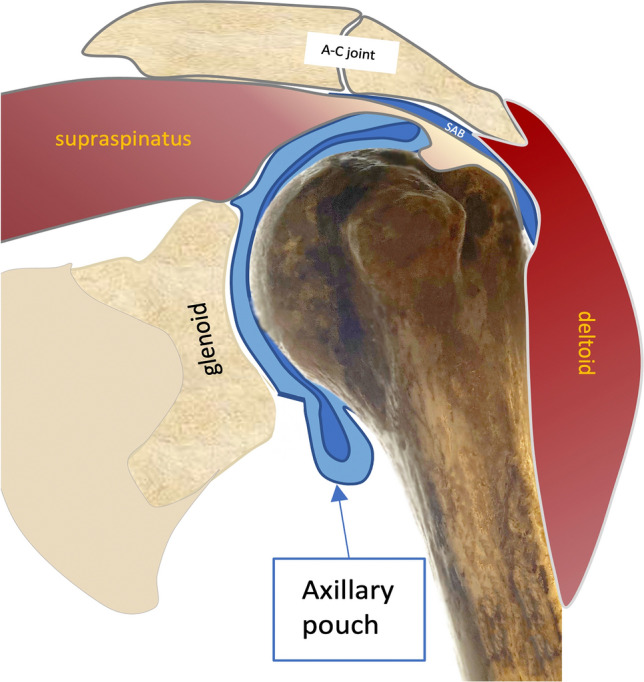
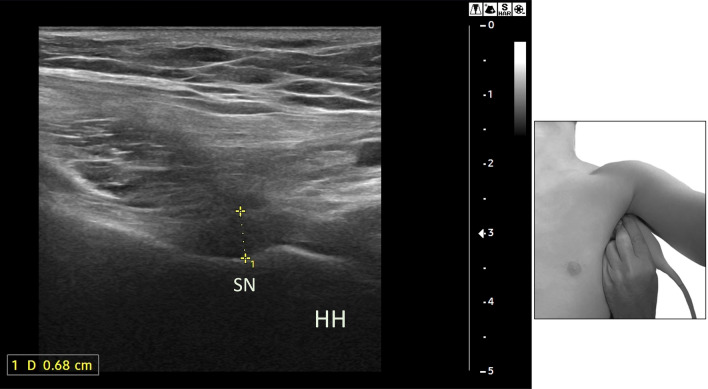
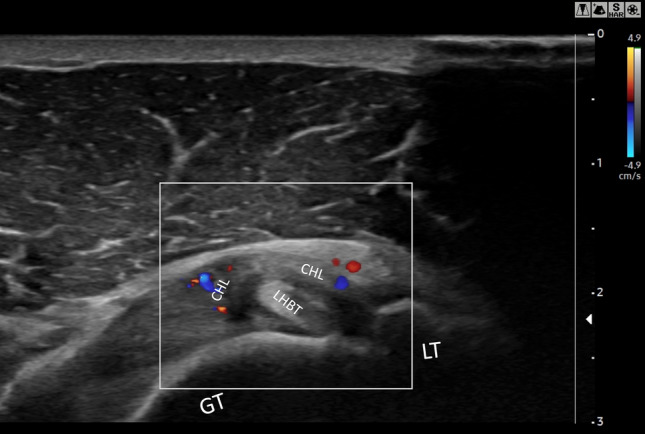
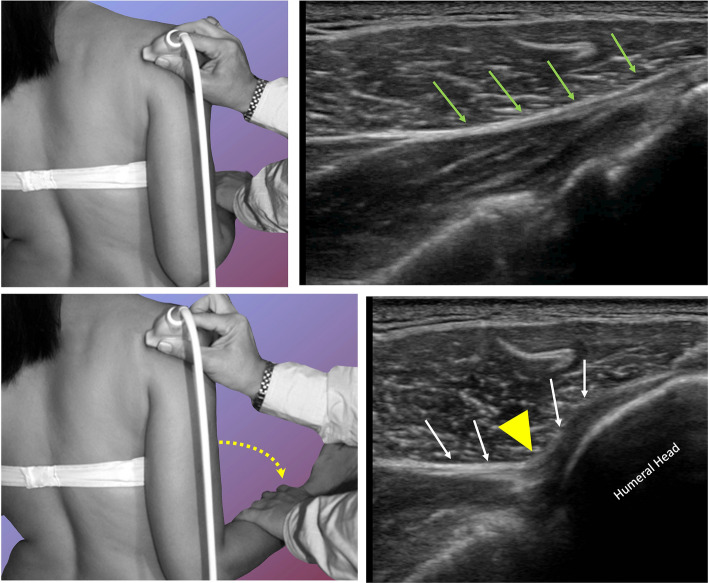
Results: We found 3723 papers on PubMed and selected those inherent to AC diagnosis, US imaging, correlation with arthroscopic and MRI findings. Forty papers which were strictly related to the topic of this narrative review were initially chosen, then 20 studies which described and exploited US for AC diagnosis were finally included. Coracohumeral ligament (2.65 ± 0.4 mm) and axillary pouch thickening (3.34 ± 0.8 mm), as well as an increase in vascularity at rotator interval (78/214, 36.44%), represented the commonest US signs useful for AC diagnosis and for which the most significant cut-off values were reported.
Conclusions: The evidence collected in this review testify that musculoskeletal US is as reliable as MRI for AC diagnosis, therefore we believe that in this context US should be considered a first-line imaging technique.
Keywords: Adhesive capsulitis; Frozen shoulder; Painful shoulder; Ultrasound.
© 2022. Società Italiana di Ultrasonologia in Medicina e Biologia (SIUMB).
Conflict of interest statement
The authors deny any conflict of interest.
Figures

References
-
- Codman EA (1934) The shoulder: rupture of the supraspinatus tendon and other lesions in or about the subacromial bursa. Thomas Todd Co., Boston
-
- Neviaser JS. Adhesive capsulitis of the shoulder. J Bone Jt Surg Am. 1945;27(2):211.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
