

Cyclic workflow to improve implementation of learning points from morbidity and mortality meetings
- PMID: 36284295
- PMCID: PMC9593980
- DOI: 10.1186/s12913-022-08639-2
Cyclic workflow to improve implementation of learning points from morbidity and mortality meetings
Abstract
Background: Morbidity and mortality meetings (M&MMs) are organized in most hospital departments with an educational purpose to learn from adverse events (AEs) to improve patient care. M&MMs often lack effectiveness due to unsuccessful systematic follow-up of areas of improvement. This can have an effect on improving patient safety and care. Therefore, a new strategy that focuses on implementing areas of improvement into daily practice is necessary. The study aim is to see if we could improve the implementation of meeting outcomes from the M&MM by using a cyclic workflow, and which factors are important to achieve its implementation.
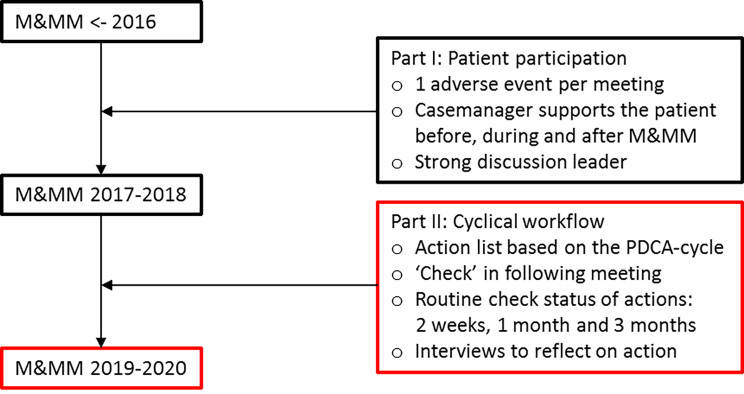
Methods: This prospective study took place at the department of gynecologic oncology of a university hospital. Research was conducted with a participatory action research (PAR) approach using 10 consecutive M&MMs in 2019 and 2020. The cyclical workflow consisted of an action list based on the PDCA-cycle, a check of the implementation of areas for improvement at the next M&MM and regular monitoring of tasks. Each M&MM was observed and each professional with an assigned task was interviewed and gave their informed consent. Thematic content analysis was performed with the program Atlas.ti 8.4.20.
Results: Out of the 39 tasks that resulted from 10 M&MMs, 37 (94.8%) followed all the steps in the PDCA-cycle and were implemented. In total, 16 interviews were conducted with consultants, nurses, registrars and residents. Five main factors were important to achieve follow-up of areas for improvement: organizational culture, motivation, commitment, communication to mobilize employees and skills. Repetition of the cyclic workflow at the M&MM and an external person who reminded professionals of their assigned task(s) was important to change habits and motivate professionals.
Conclusion: Cyclical tools can support the implementation of areas for improvement to optimize the M&MM. A M&MM with an organizational culture where attendees can discuss openly and freely may motivate attendees to take on tasks successfully. A positive stimulant to reach commitment of professionals is team participation. Integrating new habits of reflection may lead to a deeper level of learning from the PDCA-cycle and of the M&MM. Creating a learning environment outside of the M&MM may support professionals to take on actions and engage in improvement practices. Future research may focus on including a comparative analysis to show a success rate of the implementation of learning points from the M&MM more clearly.
Keywords: Complications; Group meeting; Healthcare quality; Learning; Organizational change; Patient participation; Workflow.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Openness to new perspectives created by patient participation at the morbidity and mortality meeting.Patient Educ Couns. 2021 Feb;104(2):343-351. doi: 10.1016/j.pec.2020.08.008. Epub 2020 Sep 8. Patient Educ Couns. 2021. PMID: 33051126
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
The patient experience of patient-centered communication with nurses in the hospital setting: a qualitative systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):76-87. doi: 10.11124/jbisrir-2015-1072. JBI Database System Rev Implement Rep. 2015. PMID: 26447009
-
Systematic Review of Morbidity and Mortality Meeting Standardization: Does It Lead to Improved Professional Development, System Improvements, Clinician Engagement, and Enhanced Patient Safety Culture?J Patient Saf. 2024 Mar 1;20(2):125-130. doi: 10.1097/PTS.0000000000001184. Epub 2023 Nov 30. J Patient Saf. 2024. PMID: 38038688
-
Making the most of a Morbidity and Mortality meeting.Int J Risk Saf Med. 2023;34(2):145-154. doi: 10.3233/JRS-210077. Int J Risk Saf Med. 2023. PMID: 36189607 Review.
Cited by
-
Enhancing capability for continuous organisational improvement and learning in healthcare organisations: a systematic review of the literature 2013-2022.BMJ Open Qual. 2024 Apr 2;13(2):e002566. doi: 10.1136/bmjoq-2023-002566. BMJ Open Qual. 2024. PMID: 38569667 Free PMC article.
References
-
- Mitchell EL, Lee DY, Arora S, et al. Improving the quality of the surgical morbidity and mortality conference: a prospective intervention study. Acad Med. 2013;88(6):824 – 30. - PubMed
-
- de Vos MS, Marang-van de Mheen PJ, Smith AD, et al. Toward best practices for surgical morbidity and mortality conferences: A mixed methods study. J Surg Educ. 2018;75(1):33–42. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
