

Effect of esophageal cooling on ablation lesion formation in the left atrium: Insights from Ablation Index data in the IMPACT trial and clinical outcomes
- PMID: 36284450
- PMCID: PMC10091801
- DOI: 10.1111/jce.15717
Effect of esophageal cooling on ablation lesion formation in the left atrium: Insights from Ablation Index data in the IMPACT trial and clinical outcomes
Abstract
Introduction: The IMPACT study established the role of controlled esophageal cooling in preventing esophageal thermal injury during radiofrequency (RF) ablation for atrial fibrillation (AF). The effect of esophageal cooling on ablation lesion delivery and procedural and patient outcomes had not been previously studied. The objective was to determine the effect of esophageal cooling on the formation of RF lesions, the ability to achieve procedural endpoints, and clinical outcomes.
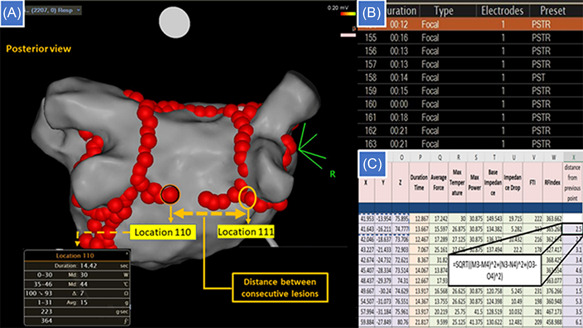
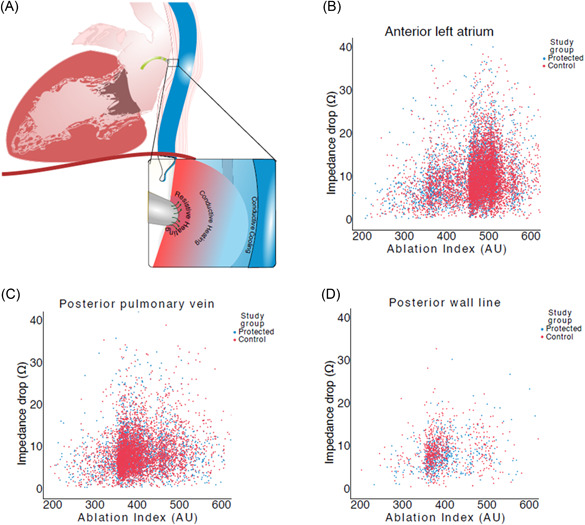
Methods: Participants in the IMPACT trial underwent AF ablation guided by Ablation Index (30 W at 350-400 AI posteriorly, 40 W at ≥450 AI anteriorly). A blinded 1:1 randomization assigned patients to the use of the ensoETM® device to keep esophageal temperature at 4°C during ablation or standard practice using a single-sensor temperature probe. Ablation parameters and clinical outcomes were analyzed.
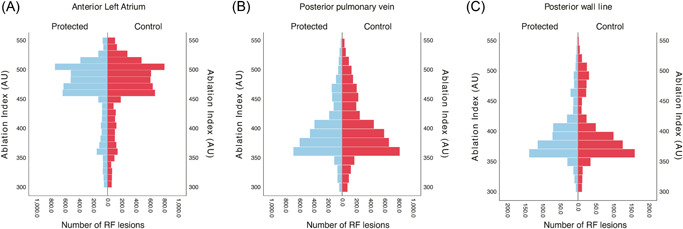
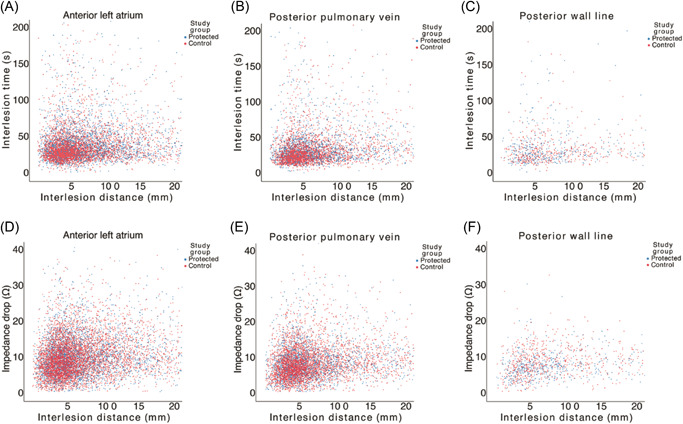
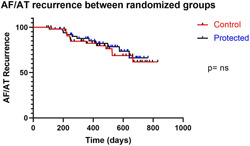
Results: Procedural data from 188 patients were analyzed. Procedure and fluoroscopy times were similar, and all pulmonary veins were isolated. First-pass pulmonary vein isolation and reconnection at the end of the waiting period were similar in both randomized groups (51/64 vs. 51/68; p = 0.54 and 5/64 vs. 7/68; p = 0.76, respectively). Posterior wall isolation was also similar: 24/33 versus 27/38; p = 0.88. Ablation effect on tissue, measured in impedance drop, was no different between the two randomized groups: 8.6Ω (IQR: 6-11.8) versus 8.76Ω (IQR: 6-12.2; p = 0.25). Arrhythmia recurrence was similar after 12 months (21.1% vs. 24.1%; 95% CI: 0.38-1.84; HR: 0.83; p = 0.66).
Conclusions: Esophageal cooling has been shown to be effective in reducing ablation-related thermal injury during RF ablation. This protection does not compromise standard procedural endpoints or clinical success at 12 months.
Keywords: AF ablation; Ablation Index; efficacy; efficiency; esophageal cooling.
© 2022 The Authors. Journal of Cardiovascular Electrophysiology published by Wiley Periodicals LLC.
Figures
Comment in
-
Esophageal cooling during radiofrequency ablation: Can opposite (strategies) attract?J Cardiovasc Electrophysiol. 2022 Dec;33(12):2558-2559. doi: 10.1111/jce.15718. Epub 2022 Nov 3. J Cardiovasc Electrophysiol. 2022. PMID: 36284448 No abstract available.
References
-
- Kapur S, Barbhaiya C, Deneke T, Michaud GF. Esophageal injury and atrioesophageal fistula caused by ablation for atrial fibrillation. Circulation. 2017;136:1247‐1255. - PubMed
-
- Hussein A, Das M, Riva S, et al. Use of ablation index‐guided ablation results in high rates of durable pulmonary vein isolation and freedom from arrhythmia in persistent atrial fibrillation patients. The PRAISE study results. Circ Arrhythm Electrophysiol. 2018;11:e006576. - PubMed
-
- Solimene F, Lepillier A, Ruvo E, et al. Reproducibility of acute pulmonary vein isolation guided by the ablation index. Pacing Clin Electrophysiol. 2019;42:874‐881. - PubMed
-
- Das M, Loveday JJ, Wynn GJ, et al. Ablation index, a novel marker of ablation lesion quality: prediction of pulmonary vein reconnection at repeat electrophysiology study and regional differences in target values. Europace. 2017;19:775‐783. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
