

Emphysematous osteomyelitis of the spine: a case report and case based review of the literature
- PMID: 36285094
- PMCID: PMC9547692
- DOI: 10.21037/jss-22-6
Emphysematous osteomyelitis of the spine: a case report and case based review of the literature
Abstract
Background/objective: Emphysematous osteomyelitis (EO) of the spine is an uncommon type of osteomyelitis characterized by intraosseous gas-formation in the vertebrae. The objective of this report is to present a rare case of spine EO in a patient with emphysematous cystitis. A case-based review of the literature on spinal EO was also performed as an update to the relevant literature of this rare infection.
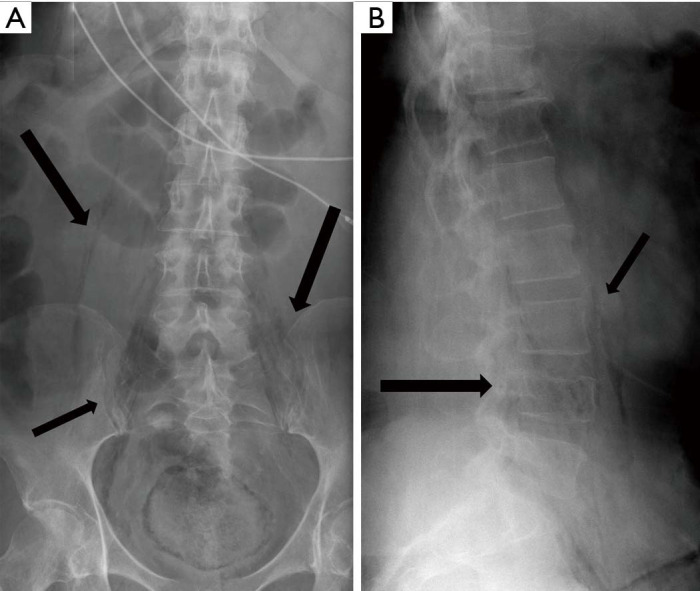
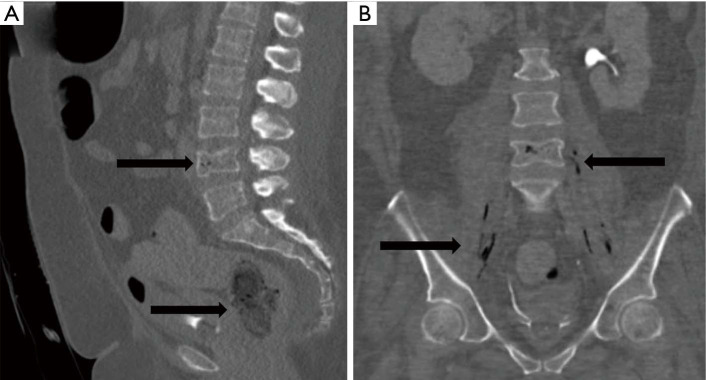
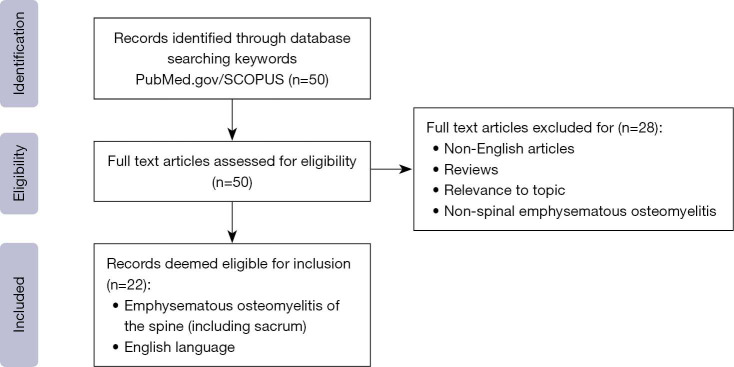
Case description/methods: A 55-year-old female with diabetes mellitus and peripheral vascular disease (PVD) presented to our institution with recurrent falls, fatigue, and low back pain. Computed tomography (CT) and magnetic resonance imaging (MRI) scans confirmed emphysematous cystitis and EO at L4. Given the diffuse involvement, surgical intervention was deferred for IV antibiotic therapy. A case-based review was also conducted by searching the SCOPUS and PubMed databases for the following terms: "emphysematous osteomyelitis", "gas", and "spine". Only publications in English were included in this review.
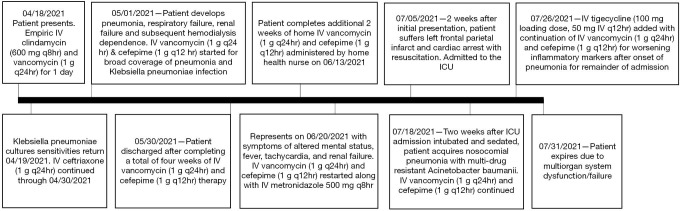
Key content/findings: Urine/blood cultures identified Klebsiella pneumoniae. After initial improvement with six weeks of broad-spectrum antibiotics, the patient re-presented with recurrent fevers and fatigue. Despite maximal medical therapy, the patient expired 2 months later due to multi-organ system failure. Including the present report, only 29 cases of spine EO have been described in the literature. Patients almost consistently presented with fever, elevated inflammatory markers, and localized pain. Most cases of spinal EO (89.7%) were monomicrobial. Escherichia coli (37.9%) and Klebsiella pneumoniae (27.6%) were the most causative organisms identified. Medical treatment universally consisted of broad-spectrum IV antibiotics prior to tailoring. Debridement and decompression, with or without fusion, were the main operative procedures performed for spine EO. Outcomes following spinal EO are varied with a 44.4% mortality rate.
Conclusions: We present a case of EO of the spine and concomitant emphysematous cystitis with Klebsiella pneumoniae and a case-based review of the literature. Appropriate work up for this rare infection should include inflammatory markers, cultures, and CT/MRI imaging. Treatment consists of IV antibiotics with anaerobic and gram-negative coverage. However, treatment guidelines and operative indications for spinal emphysematous osteomyelitis remain unclear.
Keywords: Emphysematous; case report; osteomyelitis; review; spine.
2022 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jss.amegroups.com/article/view/10.21037/jss-22-6/coif). JPG consults for device feedback and suggestions, academic conferences/travel/continuing medical education from NuVasive, Depuy Synthes; research support for materials from Nuvasive. The other authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources