

Impact of the COVID-19 pandemic on TB services at ART programmes in low- and middle-income countries: a multi-cohort survey
- PMID: 36285602
- PMCID: PMC9597377
- DOI: 10.1002/jia2.26018
Impact of the COVID-19 pandemic on TB services at ART programmes in low- and middle-income countries: a multi-cohort survey
Abstract
Introduction: COVID-19 stretched healthcare systems to their limits, particularly in settings with a pre-existing high burden of infectious diseases, including HIV and tuberculosis (TB). We studied the impact of COVID-19 on TB services at antiretroviral therapy (ART) clinics in low- and middle-income countries.
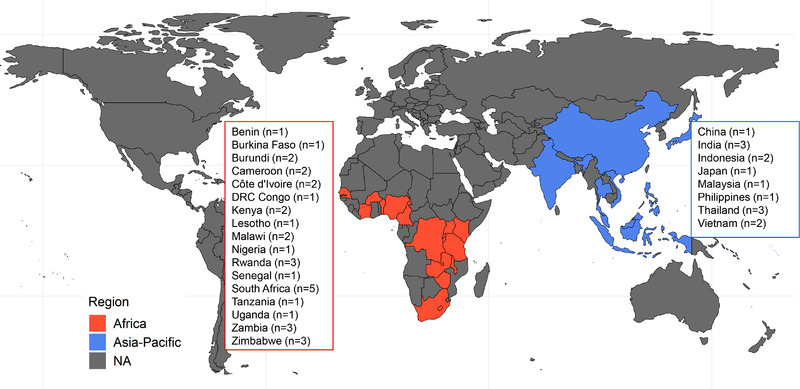
Methods: We surveyed ART clinics providing TB services in the International Epidemiology Databases to Evaluate AIDS (IeDEA) consortium in Africa and the Asia-Pacific until July 2021 (TB diagnoses until the end of 2021). We collected site-level data using standardized questionnaires.
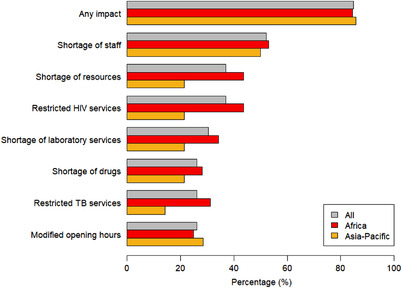
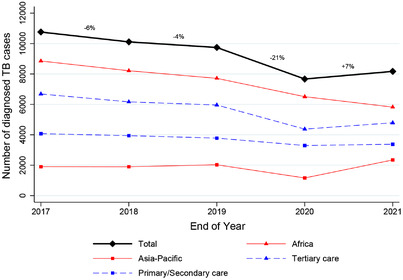
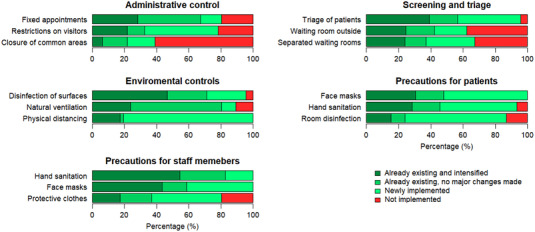
Results: Of 46 participating ART clinics, 32 (70%) were in Africa and 14 (30%) in the Asia-Pacific; 52% provided tertiary care. Most clinics (85%) reported disrupted routine HIV care services during the pandemic, both in Africa (84%) and the Asia-Pacific (86%). The most frequently reported impacts were on staff (52%) and resource shortages (37%; protective clothing, face masks and disinfectants). Restrictions in TB health services were observed in 12 clinics (26%), mainly reduced access to TB diagnosis and postponed follow-up visits (6/12, 50% each), and restrictions in TB laboratory services (22%). Restrictions of TB services were addressed by dispensing TB drugs for longer periods than usual (7/12, 58%), providing telehealth services (3/12, 25%) and with changes in directly observed therapy (DOT) (e.g. virtual DOT, 3/12). The number of TB diagnoses at participating clinics decreased by 21% in 2020 compared to 2019; the decline was more pronounced in tertiary than primary/secondary clinics (24% vs. 12%) and in sites from the Asia-Pacific compared to Africa (46% vs. 14%). In 2021, TB diagnoses continued to decline in Africa (-8%) but not in the Asia-Pacific (+62%) compared to 2020. During the pandemic, new infection control measures were introduced or intensified at the clinics, including wearing face masks, hand sanitation and patient triage.
Conclusions: The COVID-19 pandemic led to staff shortages, reduced access to TB care and delays in follow-up visits for people with TB across IeDEA sites in Africa and the Asia-Pacific. Increased efforts are needed to restore and secure ongoing access to essential TB services in these contexts.
Keywords: COVID-19; HIV clinic; antiretroviral therapy; differentiated service delivery; low- and middle-income countries; tuberculosis.
© 2022 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Conflict of interest statement
None to declare.
Figures
Similar articles
-
The long-term impact of the COVID-19 pandemic on tuberculosis care and infection control measures in anti-retroviral therapy (ART) clinics in low- and middle-income countries: a multiregional site survey in Asia and Africa.BMJ Glob Health. 2025 Mar 24;10(3):e017828. doi: 10.1136/bmjgh-2024-017828. BMJ Glob Health. 2025. PMID: 40127942 Free PMC article.
-
Characteristics and comprehensiveness of adult HIV care and treatment programmes in Asia-Pacific, sub-Saharan Africa and the Americas: results of a site assessment conducted by the International epidemiologic Databases to Evaluate AIDS (IeDEA) Collaboration.J Int AIDS Soc. 2014 Dec 15;17(1):19045. doi: 10.7448/IAS.17.1.19045. eCollection 2014. J Int AIDS Soc. 2014. PMID: 25516092 Free PMC article.
-
COVID-19 associated changes in HIV service delivery over time in Central Africa: Results from facility surveys during the first and second waves of the pandemic.PLoS One. 2022 Nov 30;17(11):e0275429. doi: 10.1371/journal.pone.0275429. eCollection 2022. PLoS One. 2022. PMID: 36449454 Free PMC article.
-
Interventions to improve linkage along the HIV-tuberculosis care cascades in low- and middle-income countries: A systematic review and meta-analysis.PLoS One. 2022 May 12;17(5):e0267511. doi: 10.1371/journal.pone.0267511. eCollection 2022. PLoS One. 2022. PMID: 35552547 Free PMC article.
-
Triple Burden: The Incorrigible Threat of Tuberculosis, HIV, and COVID-19.Infect Disord Drug Targets. 2024;24(4):1-7. doi: 10.2174/0118715265259959231031104820. Infect Disord Drug Targets. 2024. PMID: 37937570 Review.
Cited by
-
COVID-19 policies and tuberculosis services in private health sectors of India, Indonesia, and Nigeria.J Clin Tuberc Other Mycobact Dis. 2024 Dec 2;38:100503. doi: 10.1016/j.jctube.2024.100503. eCollection 2025 Feb. J Clin Tuberc Other Mycobact Dis. 2024. PMID: 39758563 Free PMC article.
-
The Tuberculosis Sentinel Research Network (TB-SRN) of the International epidemiology Databases to Evaluate AIDS (IeDEA): protocol for a prospective cohort study in Africa, Southeast Asia and Latin America.BMJ Open. 2024 Jan 9;14(1):e079138. doi: 10.1136/bmjopen-2023-079138. BMJ Open. 2024. PMID: 38195167 Free PMC article.
-
Infection prevention and control measures during the COVID-19 pandemic and airborne tuberculosis transmission during primary care visits in South Africa.Int J Infect Dis. 2025 Jul;156:107921. doi: 10.1016/j.ijid.2025.107921. Epub 2025 May 6. Int J Infect Dis. 2025. PMID: 40339785 Free PMC article.
-
Impact of the SARS-COV-2 pandemic on access to health services in Angola: a focus on diagnosis and treatment services for tuberculosis.Front Public Health. 2025 Apr 24;13:1530782. doi: 10.3389/fpubh.2025.1530782. eCollection 2025. Front Public Health. 2025. PMID: 40342501 Free PMC article.
-
"I pity the TB patient": a mixed methods study assessing the impact of the COVID-19 pandemic on TB services in two major Indonesian cities and distilling lessons for the future.BMJ Glob Health. 2024 May 16;9(5):e014943. doi: 10.1136/bmjgh-2023-014943. BMJ Glob Health. 2024. PMID: 38760026 Free PMC article.
References
-
- World Health Organization . Global Tuberculosis Report 2019. 2020 [cited 2022 Mar 10]. Available from: https://apps.who.int/iris/rest/bitstreams/1312164/retrieve
-
- World Health Organization . WHO Coronavirus (COVID‐19) Dashboard. [cited 2022 Apr 6]. Available from: https://covid19.who.int
