

Effect of Selective Decontamination of the Digestive Tract on Hospital Mortality in Critically Ill Patients Receiving Mechanical Ventilation: A Randomized Clinical Trial
- PMID: 36286097
- PMCID: PMC9607966
- DOI: 10.1001/jama.2022.17927
Effect of Selective Decontamination of the Digestive Tract on Hospital Mortality in Critically Ill Patients Receiving Mechanical Ventilation: A Randomized Clinical Trial
Abstract
Importance: Whether selective decontamination of the digestive tract (SDD) reduces mortality in critically ill patients remains uncertain.
Objective: To determine whether SDD reduces in-hospital mortality in critically ill adults.
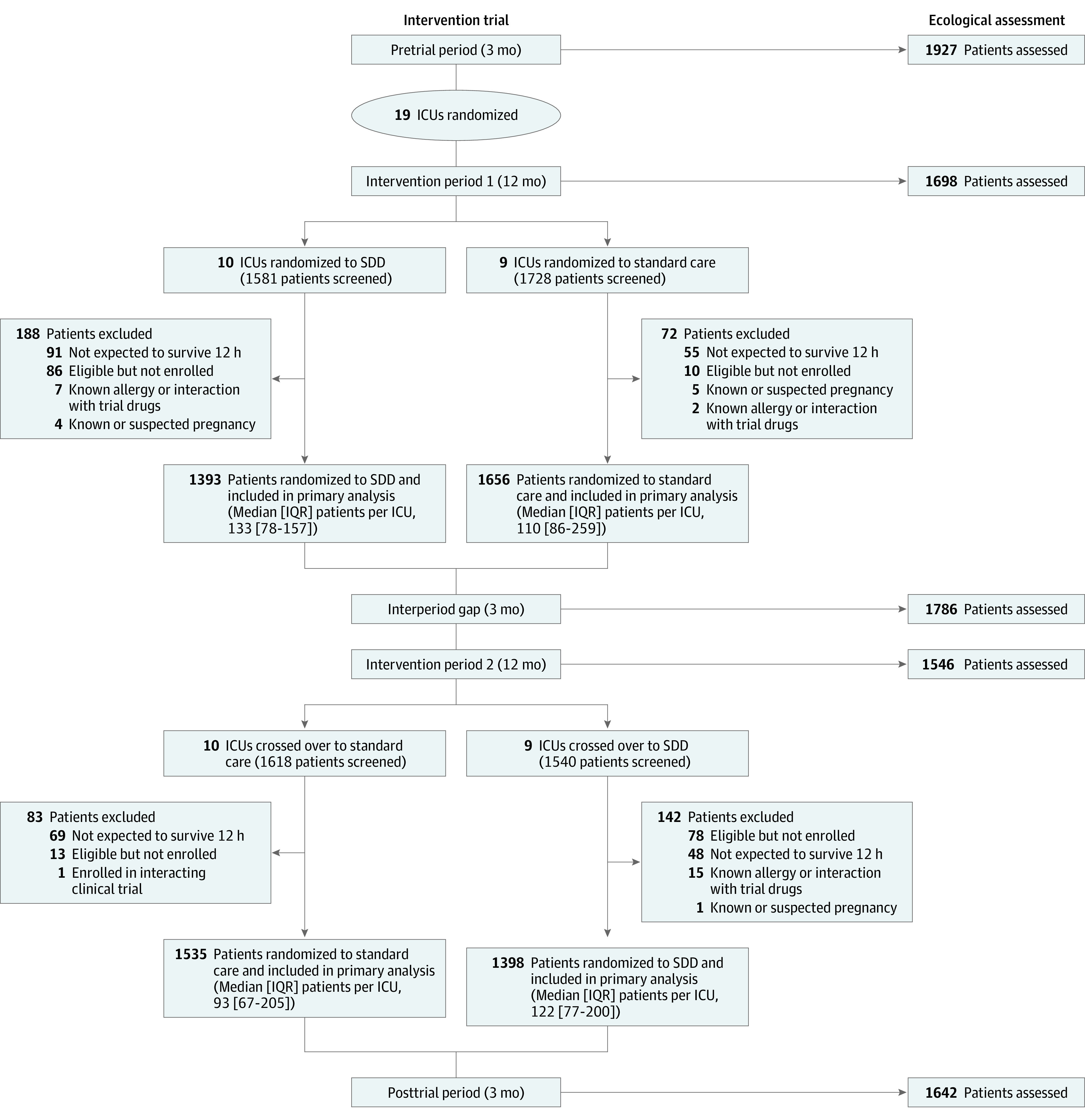
Design, setting, and participants: A cluster, crossover, randomized clinical trial that recruited 5982 mechanically ventilated adults from 19 intensive care units (ICUs) in Australia between April 2018 and May 2021 (final follow-up, August 2021). A contemporaneous ecological assessment recruited 8599 patients from participating ICUs between May 2017 and August 2021.
Interventions: ICUs were randomly assigned to adopt or not adopt a SDD strategy for 2 alternating 12-month periods, separated by a 3-month interperiod gap. Patients in the SDD group (n = 2791) received a 6-hourly application of an oral paste and administration of a gastric suspension containing colistin, tobramycin, and nystatin for the duration of mechanical ventilation, plus a 4-day course of an intravenous antibiotic with a suitable antimicrobial spectrum. Patients in the control group (n = 3191) received standard care.
Main outcomes and measures: The primary outcome was in-hospital mortality within 90 days. There were 8 secondary outcomes, including the proportion of patients with new positive blood cultures, antibiotic-resistant organisms (AROs), and Clostridioides difficile infections. For the ecological assessment, a noninferiority margin of 2% was prespecified for 3 outcomes including new cultures of AROs.
Results: Of 5982 patients (mean age, 58.3 years; 36.8% women) enrolled from 19 ICUs, all patients completed the trial. There were 753/2791 (27.0%) and 928/3191 (29.1%) in-hospital deaths in the SDD and standard care groups, respectively (mean difference, -1.7% [95% CI, -4.8% to 1.3%]; odds ratio, 0.91 [95% CI, 0.82-1.02]; P = .12). Of 8 prespecified secondary outcomes, 6 showed no significant differences. In the SDD vs standard care groups, 23.1% vs 34.6% had new ARO cultures (absolute difference, -11.0%; 95% CI, -14.7% to -7.3%), 5.6% vs 8.1% had new positive blood cultures (absolute difference, -1.95%; 95% CI, -3.5% to -0.4%), and 0.5% vs 0.9% had new C difficile infections (absolute difference, -0.24%; 95% CI, -0.6% to 0.1%). In 8599 patients enrolled in the ecological assessment, use of SDD was not shown to be noninferior with regard to the change in the proportion of patients who developed new AROs (-3.3% vs -1.59%; mean difference, -1.71% [1-sided 97.5% CI, -∞ to 4.31%] and 0.88% vs 0.55%; mean difference, -0.32% [1-sided 97.5% CI, -∞ to 5.47%]) in the first and second periods, respectively.
Conclusions and relevance: Among critically ill patients receiving mechanical ventilation, SDD, compared with standard care without SDD, did not significantly reduce in-hospital mortality. However, the confidence interval around the effect estimate includes a clinically important benefit.
Trial registration: ClinicalTrials.gov Identifier: NCT02389036.
Conflict of interest statement
Figures


Comment in
-
Selective Decontamination of the Digestive Tract: An Answer at Last?JAMA. 2022 Dec 20;328(23):2310-2311. doi: 10.1001/jama.2022.18623. JAMA. 2022. PMID: 36378275 No abstract available.
-
Selective Decontamination of the Digestive Tract and Hospital Mortality in Critically Ill Patients Receiving Mechanical Ventilation.JAMA. 2023 Mar 28;329(12):1029. doi: 10.1001/jama.2023.0221. JAMA. 2023. PMID: 36976285 No abstract available.
-
Selective Decontamination of the Digestive Tract and Hospital Mortality in Critically Ill Patients Receiving Mechanical Ventilation.JAMA. 2023 Mar 28;329(12):1029-1030. doi: 10.1001/jama.2023.0218. JAMA. 2023. PMID: 36976286 No abstract available.
-
Infectious Diseases in the ICU: Studies on Prevention and Treatment.Am J Respir Crit Care Med. 2025 Feb;211(2):258-260. doi: 10.1164/rccm.202405-1090RR. Am J Respir Crit Care Med. 2025. PMID: 39586002 No abstract available.
References
-
- Stoutenbeek CP, van Saene HK, Little RA, Whitehead A; Working Group on Selective Decontamination of the Digestive Tract . The effect of selective decontamination of the digestive tract on mortality in multiple trauma patients: a multicenter randomized controlled trial. Intensive Care Med. 2007;33(2):261-270. doi: 10.1007/s00134-006-0455-4 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
