

Predictive Value of the Transthoracic Echocardiography Index for Acute Kidney Injury after Cardiac Valve Surgery
- PMID: 36286268
- PMCID: PMC9604519
- DOI: 10.3390/jcdd9100316
Predictive Value of the Transthoracic Echocardiography Index for Acute Kidney Injury after Cardiac Valve Surgery
Abstract
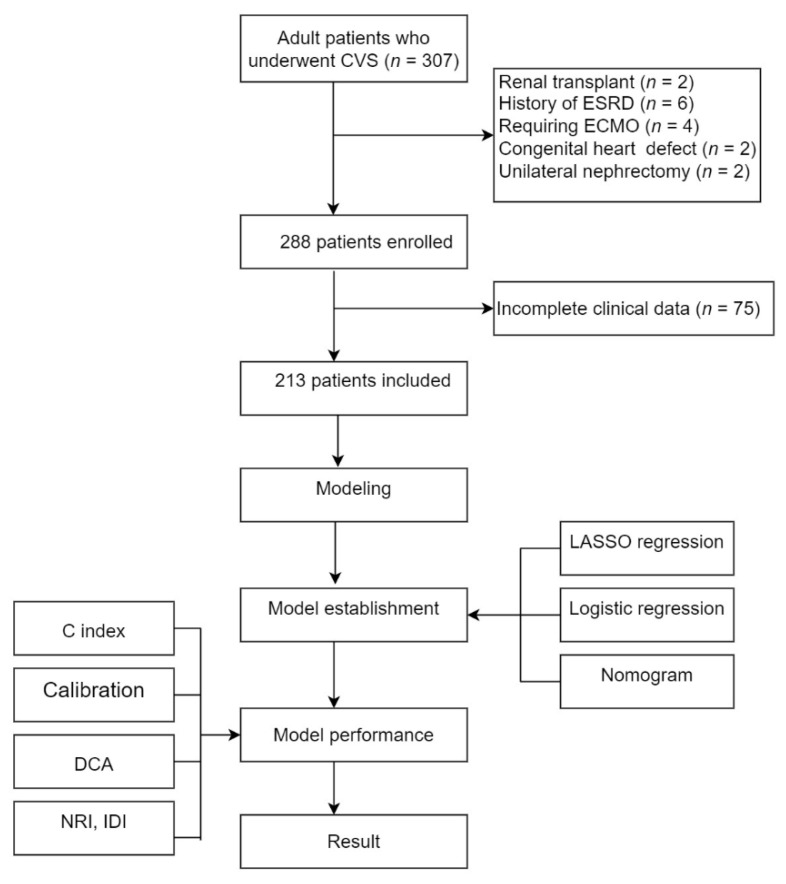
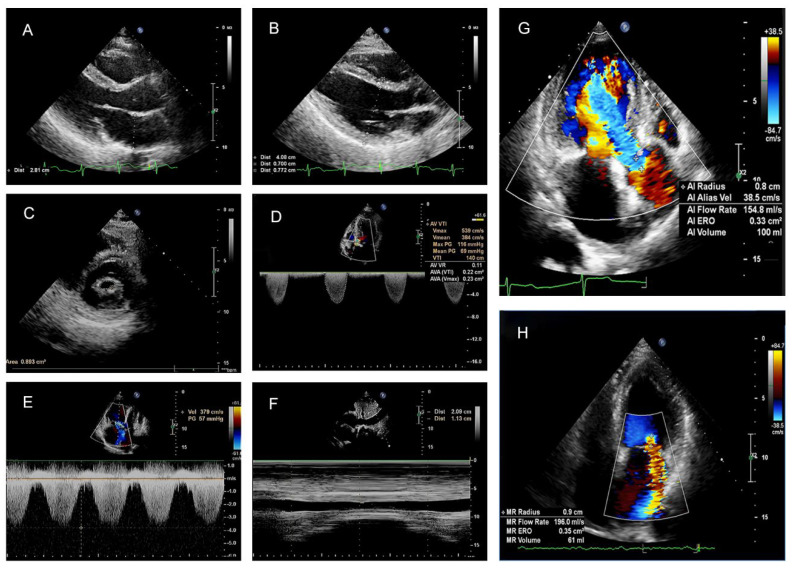
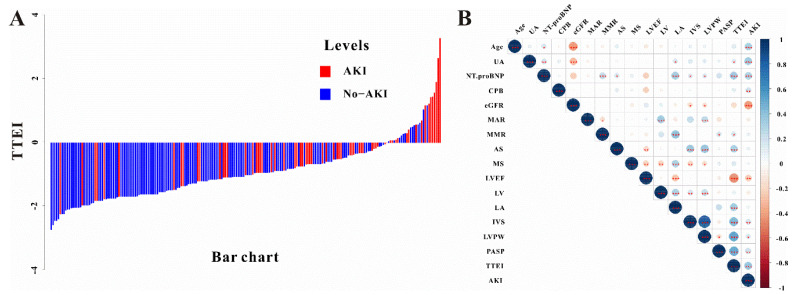
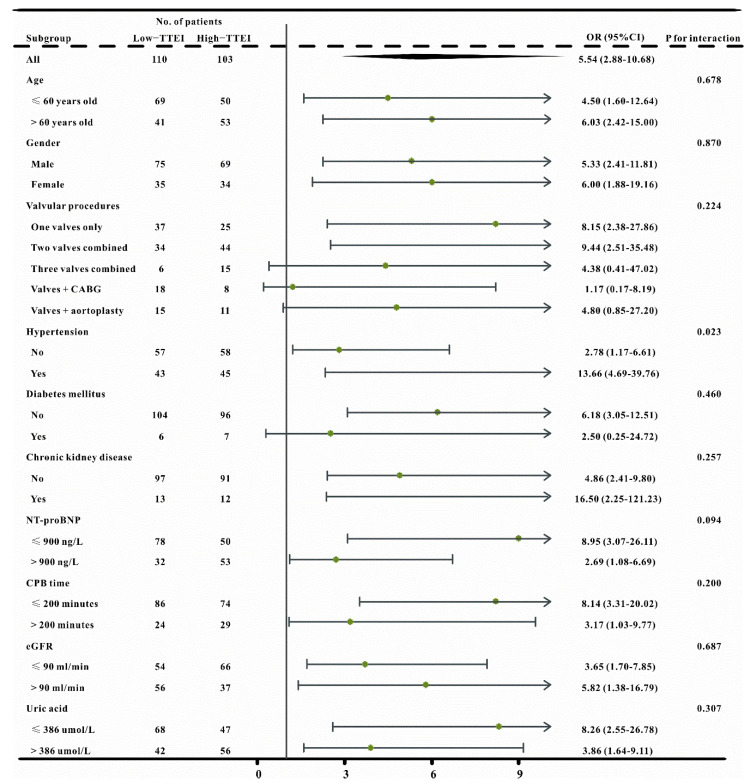
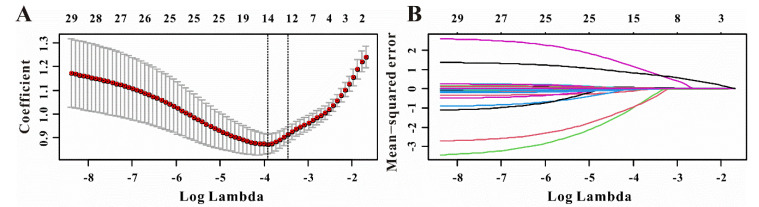
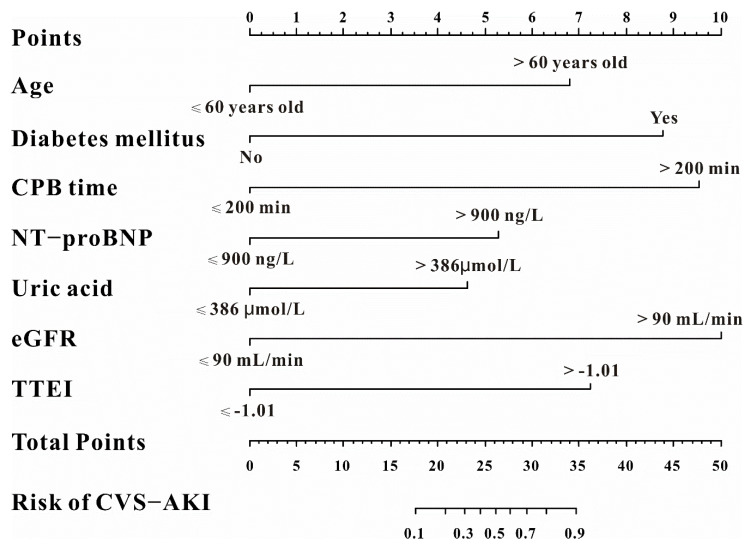
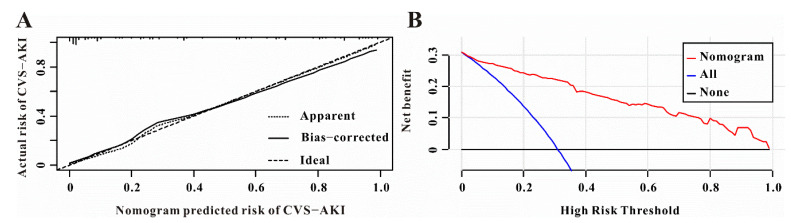
Background: We aimed to demonstrate whether the preoperative transthoracic echocardiography index (TTEI) could improve the predictive value of clinical parameters for cardiac valve surgery-associated acute kidney injury (CVS−AKI). Methods: A total of 213 patients who underwent surgical CVS at Renmin Hospital of Wuhan University were consecutively recruited in this retrospective study. TTE assessments were performed within 7 days before surgery and logistic regression was used to determine TTEI. A nomogram was constructed by integrating TTEI and clinical features, and the net reclassification index (NRI) and integrated discrimination improvement (IDI) were applied to evaluate the improvement in TTEI for CVS−AKI. Results: Among them, 66 patients (30.9%) developed CVS−AKI. The TTEI was calculated as follows: −6.579 + 0.068 × pulmonary artery systolic pressure (mmHg) −0.742 × LVEF (>55%, yes or no) + 0.346 × left ventricle posterior wall thickness (mm). The nomogram based on the TEEI and other clinical factors possessed excellent performance (C-index = 0.880), had great calibration and discrimination, and was clinically useful. Furthermore, NRI (0.07, 95% confidence interval, 95%CI, 0.01−0.12, p = 0.02) and IDI (0.08, 95%CI, 0.01−0.20, p = 0.02) indicated that TTEI could significantly improve the predictive value of clinical features for CVS−AKI. Conclusions: As a simple access and cost-effective parameter, the preoperative TTEI may be a reliable and useful factor for CVS−AKI.
Keywords: acute kidney injury; cardiac valve surgery; nomogram; risk assessment; transthoracic echocardiography index.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Predictive Value of Glycosylated Hemoglobin for Post-operative Acute Kidney Injury in Non-cardiac Surgery Patients.Front Med (Lausanne). 2022 Jul 11;9:886210. doi: 10.3389/fmed.2022.886210. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35899215 Free PMC article.
-
Preoperative NT-proBNP and LVEF for the prediction of acute kidney injury after noncardiac surgery: a single-centre retrospective study.BMC Anesthesiol. 2022 Jun 24;22(1):196. doi: 10.1186/s12871-022-01727-0. BMC Anesthesiol. 2022. PMID: 35751021 Free PMC article.
-
Correlation Between Vasoactive-Inotropic Score and Postoperative Acute Kidney Injury after Cardiovascular Surgery.Heart Surg Forum. 2021 Mar 25;24(2):E282-E292. doi: 10.1532/hsf.3537. Heart Surg Forum. 2021. PMID: 33798050
-
Risk factors of cardiac surgery-associated acute kidney injury: development and validation of a perioperative predictive nomogram.J Nephrol. 2019 Dec;32(6):937-945. doi: 10.1007/s40620-019-00624-z. Epub 2019 Jun 26. J Nephrol. 2019. PMID: 31243735
-
Independent Risk Factors Contributing to Acute Kidney Injury According to Updated Valve Academic Research Consortium-2 Criteria After Transcatheter Aortic Valve Implantation: A Meta-analysis and Meta-regression of 13 Studies.J Cardiothorac Vasc Anesth. 2017 Jun;31(3):816-826. doi: 10.1053/j.jvca.2016.12.021. Epub 2016 Dec 21. J Cardiothorac Vasc Anesth. 2017. PMID: 28385646 Review.
Cited by
-
Prognostic value of transthoracic echocardiography score for the prognosis of continuous ambulatory peritoneal dialysis patients.BMC Nephrol. 2024 Feb 23;25(1):65. doi: 10.1186/s12882-024-03493-2. BMC Nephrol. 2024. PMID: 38395753 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
