

Efficacy and Safety of RBX2660 in PUNCH CD3, a Phase III, Randomized, Double-Blind, Placebo-Controlled Trial with a Bayesian Primary Analysis for the Prevention of Recurrent Clostridioides difficile Infection
- PMID: 36287379
- PMCID: PMC9607700
- DOI: 10.1007/s40265-022-01797-x
Efficacy and Safety of RBX2660 in PUNCH CD3, a Phase III, Randomized, Double-Blind, Placebo-Controlled Trial with a Bayesian Primary Analysis for the Prevention of Recurrent Clostridioides difficile Infection
Erratum in
-
Correction to: Efficacy and Safety of RBX2660 in PUNCH CD3, a Phase III, Randomized, Double-Blind, Placebo-Controlled Trial with a Bayesian Primary Analysis for the Prevention of Recurrent Clostridioides difficile Infection.Drugs. 2022 Oct;82(15):1539. doi: 10.1007/s40265-022-01805-0. Drugs. 2022. PMID: 36342618 Free PMC article. No abstract available.
Abstract
Background: Recurrent Clostridioides difficile infection, associated with dysbiosis of gut microbiota, has substantial disease burden in the USA. RBX2660 is a live biotherapeutic product consisting of a broad consortium of microbes prepared from human stool that is under investigation for the reduction of recurrent C. difficile infection.
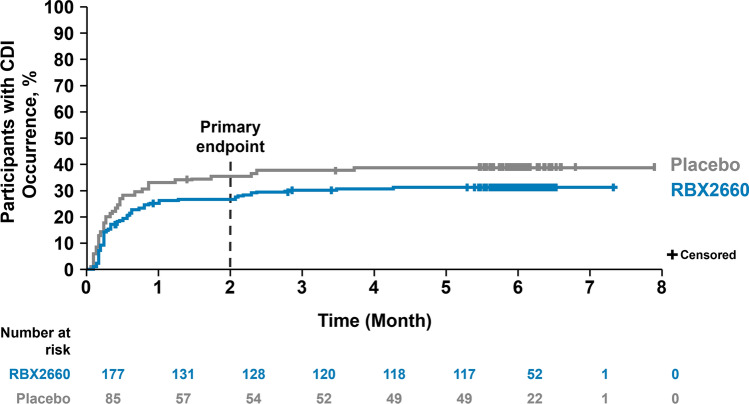
Methods: A randomized, double-blind, placebo-controlled, phase III study, with a Bayesian primary analysis integrating data from a previous phase IIb study, was conducted. Adults who had one or more C. difficile infection recurrences with a positive stool assay for C. difficile and who were previously treated with standard-of-care antibiotics were randomly assigned 2:1 to receive a subsequent blinded, single-dose enema of RBX2660 or placebo. The primary endpoint was treatment success, defined as the absence of C. difficile infection diarrhea within 8 weeks of study treatment.
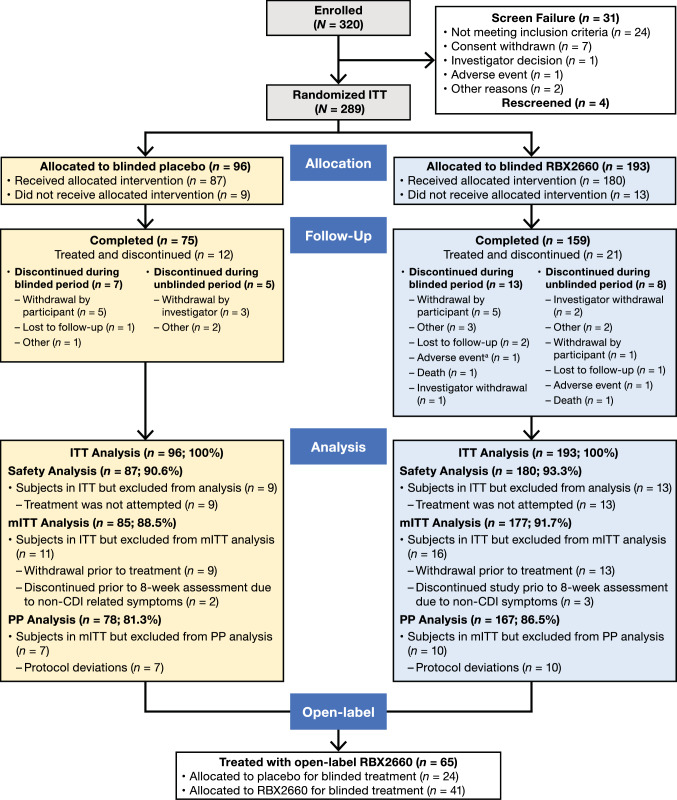
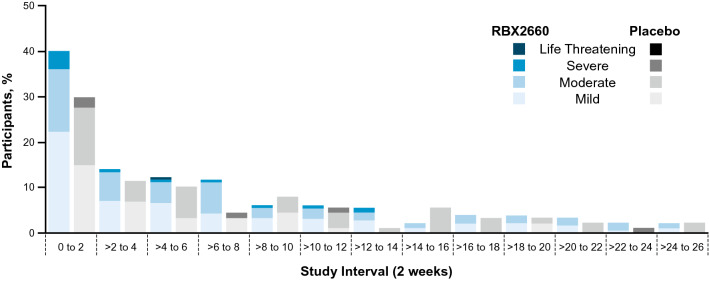
Results: Of the 320 patients screened, 289 were randomly assigned and 267 received blinded treatment (n = 180, RBX2660; n = 87, placebo). Original model estimates of treatment success were 70.4% versus 58.1% with RBX2660 and placebo, respectively. However, after aligning the data to improve the exchangeability and interpretability of the Bayesian analysis, the model-estimated treatment success rate was 70.6% with RBX2660 versus 57.5% with placebo, with an estimated treatment effect of 13.1% and a posterior probability of superiority of 0.991. More than 90% of the participants who achieved treatment success at 8 weeks had sustained response through 6 months in both the RBX2660 and the placebo groups. Overall, RBX2660 was well tolerated, with manageable adverse events. The incidence of treatment-emergent adverse events was higher in RBX2660 recipients compared with placebo and was mostly driven by a higher incidence of mild gastrointestinal events.
Conclusions: RBX2660 is a safe and effective treatment to reduce recurrent C. difficile infection following standard-of-care antibiotics with a sustained response through 6 months.
Clinical trial registration: NCT03244644; 9 August, 2017.
Plain language summary
Clostridioides difficile is a diarrhea-causing bacterium that is associated with potentially serious and fatal consequences. Antibiotics used to treat or prevent infections have a side effect of damaging the healthy protective gut bacteria (microbiota). Damage to the gut microbiota can allow C. difficile to over-grow and produce toxins that injure the colon. Paradoxically, the standard of care treatment of C. difficile infection (CDI) is antibiotics. Although initially effective for the control of diarrhea, antibiotics can leave a patient at risk for CDI recurrence after antibiotic treatment is stopped. Live biotherapeutic products are microbiota-based treatments used to repair the gut microbiota. These products have been shown to reduce the recurrence of CDI. RBX2660 is an investigational microbiota-based live biotherapeutic. RBX2660 contains a diverse set of microorganisms. RBX2660 has been developed to reduce CDI recurrence in adults following antibiotic treatment for recurrent CDI. This study was conducted to demonstrate that RBX2660 is effective and safe in treating patients with recurrent CDI. Treatment was considered successful in participants who did not experience CDI recurrence within 8 weeks after administration. Overall, statistical modeling demonstrated that 70.6% of participants treated with RBX2660 and 57.5% of participants treated with placebo remained free of CDI recurrence through 8 weeks. A 13.1 percentage point increase in treatment success was observed with RBX2660 treatment compared with placebo. In participants who achieved treatment success at 8 weeks, more than 90% remained free of CDI recurrence through 6 months. The most common side effects with RBX2660 treatment were abdominal pain and diarrhea. No serious treatment-related side effects were reported. The current data from the comprehensive clinical development program support a positive benefit-risk profile for RBX2660 in the reduction of CDI recurrence in adults following antibiotic therapy for recurrent CDI.
© 2022. The Author(s).
Conflict of interest statement
Sahil Khanna has received grants or contracts from Rebiotix (a Ferring company), Finch Therapeutics, Seres Therapeutics, and Vedanta BioSciences, consulting fees from Niche Pharmaceuticals and Immuron Limited, participated on advisory or data safety monitoring boards for Ferring Pharmaceuticals, and has stock options with Jetson Probiotics. Christine Lee has received grants or contracts from Rebiotix, Inc., Seres Therapeutics, and Summit Therapeutic and participated on advisory or data safety monitoring boards for Ferring Pharmaceuticals and Pfizer. Thomas Louie has received consulting fees from Crestone, MGB BioPharma, Rebiotix, Inc., and Seres Therapeutics and participated on advisory boards for Seres Therapeutics and Vedanta BioSciences. Scott M. Berry has ownership in Berry Consultants who received fees for trial design and analyses; Tricia Braun, Lindy Bancke, and Xin Su are employees of Rebiotix, Inc. or were during conduct of the study. Paul Feuerstadt has received consulting fees from Rebiotix, Inc. and Takeda Pharmaceuticals, honoraria from Ferring Pharmaceuticals, Seres Therapeutics, and Takeda Pharmaceuticals, and participated on advisory or data safety monitoring boards for Ferring Pharmaceuticals, Seres Therapeutics, and Takeda Pharmaceuticals. Humberto Aguilar, Maha Assi, Julia Garcia-Diaz, Whitfield Knapple, Gary P. Wang, and David Yoho have no conflicts of interest to declare.
Figures
References
-
- McDonald LC, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) Clin Infect Dis. 2018;66(7):e1–48. doi: 10.1093/cid/cix1085. - DOI - PMC - PubMed
-
- Johnson S, et al. Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of Clostridioides difficile infection in adults. Clin Infect Dis. 2021;73(5):e1029–e1044. doi: 10.1093/cid/ciab549. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
