

Vascular Aging and Arterial Stiffness
- PMID: 36287415
- PMCID: PMC9563886
- DOI: 10.36660/abc.20210708
Vascular Aging and Arterial Stiffness
Abstract
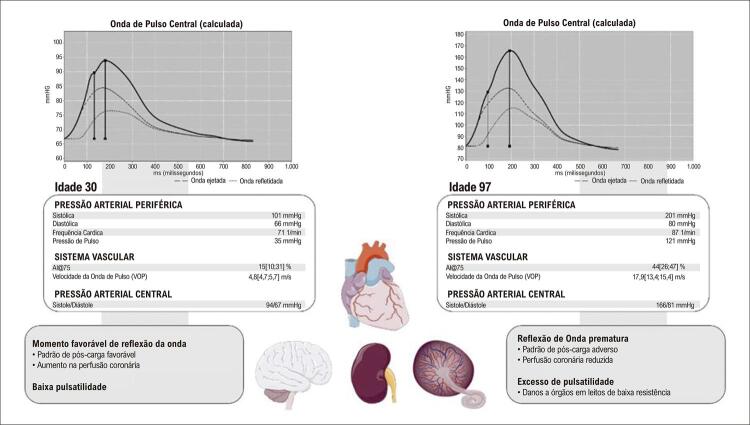
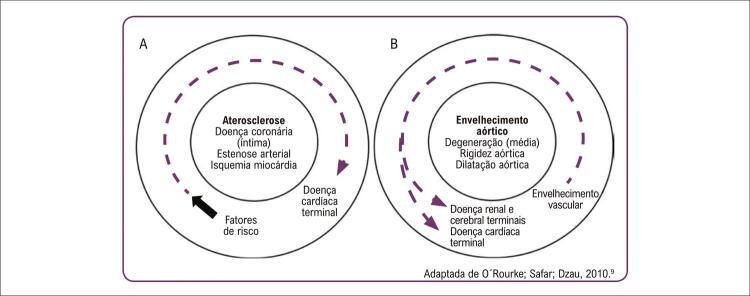
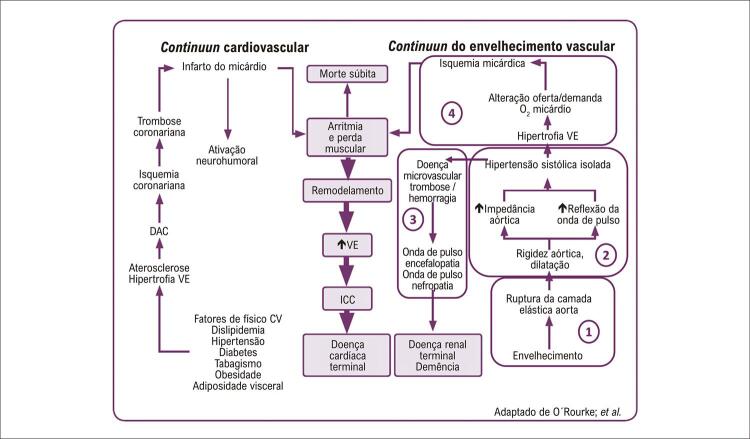
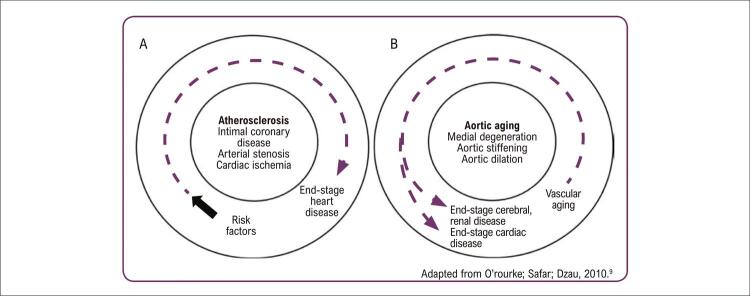
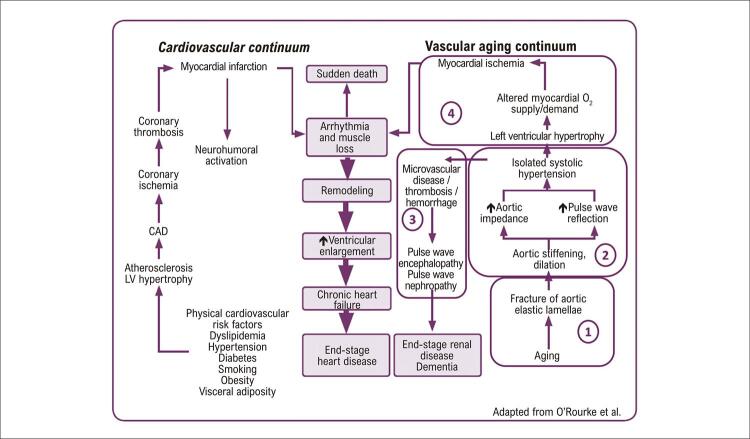
Biological aging occurs as a result of the interaction between genetics, chronological age and external factors. It is the basis for new concepts of vascular aging, whose progression is determined by the difference between biological and chronological age. From the structural point of view, the effects of vascular aging are more evident in the tunica media of large elastic arteries, marked by increased arterial stiffness, lumen dilation and wall thickness. These effects are described in the continuum of cardiovascular aging (proposed by Dzau in 2010), in which the progressive steps of microvasculature lesions of the heart, kidney and brain are initiated from the aging process. The increase of arterial stiffness can be detected by several non-invasive methods. Cardiovascular events have been traditionally described using scores that combine conventional risk factors for atherosclerosis. In the classic cardiovascular continuum (Dzau, 2006), to determine the exact contribution of each risk factor is challenging; however, since arterial stiffness reflects both early and cumulative damage of these cardiovascular risk factors, it is an indicator of the actual damage to the arterial wall. This article provides a general overview of pathophysiological mechanisms, arterial structural changes, and hemodynamic consequences of arterial stiffness; non-invasive methods for the assessment of arterial stiffness and of central blood pressure; the cardiovascular aging continuum, and the application of arterial stiffness in cardiovascular risk stratification.
O envelhecimento biológico é reflexo da interação entre genética, idade cronológica e fatores externos; é a base para novos conceitos em envelhecimento vascular, cuja progressão é determinada pela diferença entre idade biológica e cronológica. Do ponto de vista estrutural, os efeitos do envelhecimento vascular são mais evidentes na camada média das grandes artérias elásticas e resultam em aumento da rigidez arterial, da dilatação do lúmen e da espessura da parede. Esses efeitos são descritos no continuum de envelhecimento cardiovascular (proposto por Dzau em 2010) em que as etapas progressivas de lesões da microvasculatura de coração, rins e cérebro, têm início a partir do processo de envelhecimento. O aumento da rigidez arterial pode ser verificado de forma não invasiva por vários métodos. Os eventos cardiovasculares têm sido tradicionalmente previstos utilizando escores que combinam fatores de risco convencionais para aterosclerose. No continuum cardiovascular clássico (Dzau, 2006), é desafiador avaliar o peso exato da contribuição de cada fator de risco; entretanto, por refletir o dano precoce e cumulativo desses fatores de riscos cardiovascular, a rigidez arterial reflete o verdadeiro dano à parede arterial. Este artigo fornece uma visão geral dos mecanismos da fisiopatogenia, alterações estruturais das artérias e consequências hemodinâmicas do envelhecimento arterial; métodos não invasivos para a avaliação da rigidez arterial e da medida central da pressão arterial; o continuum de envelhecimento cardiovascular, e aplicação do conceito de rigidez arterial na estratificação de risco cardiovascular.
Conflict of interest statement
Potencial conflito de interesse
Não há conflito com o presente artigo
Figures




References
-
- Hamczyk MR, Nevado RM, Barettino A, Fuster V, Andrés V. Biological Versus Chronological Aging: JACC Focus Seminar. 10.1016/j.jacc.2019.11.062.J Am Coll Cardiol. 2020 Mar 3;75(8):919–930. - PubMed
-
- Barroso W, Barbosa E, Mota-Gomes A. Rigidez Arterial e Hemodinâmica Central: Do Endotélio à Camada Média. São Paulo: Athos Mais Editora; 2020.
-
- Cunha PG, Boutouyrie P, Nilsson PM, Laurent S. Early Vascular Ageing (EVA): Definitions and Clinical Applicability. 10.2174/1573402113666170413094319.Curr Hypertens Rev. 2017;13(1):8–15. - PubMed
-
- Nilsson PM, Boutouyrie P, Cunha P, Kotsis V, Narkiewicz K, Parati G, et al. Early Vascular Ageing in Translation: From Laboratory Investigations to Clinical Applications in Cardiovascular Prevention. 10.1097/HJH.0b013e328361e4bd.J Hypertens. 2013;31(8):1517–1526. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
