

A comparison of DNA sequencing and gene expression profiling to assist tissue of origin diagnosis in cancer of unknown primary
- PMID: 36287571
- PMCID: PMC10099529
- DOI: 10.1002/path.6022
A comparison of DNA sequencing and gene expression profiling to assist tissue of origin diagnosis in cancer of unknown primary
Abstract
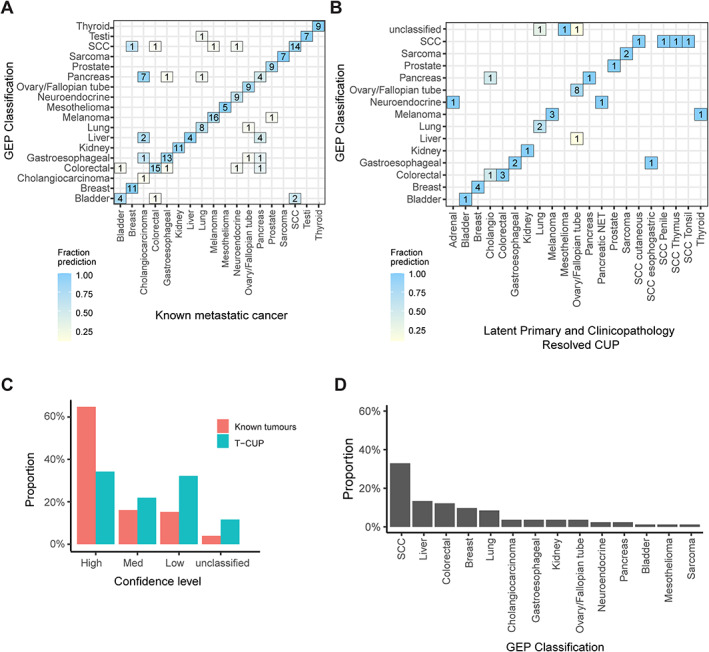
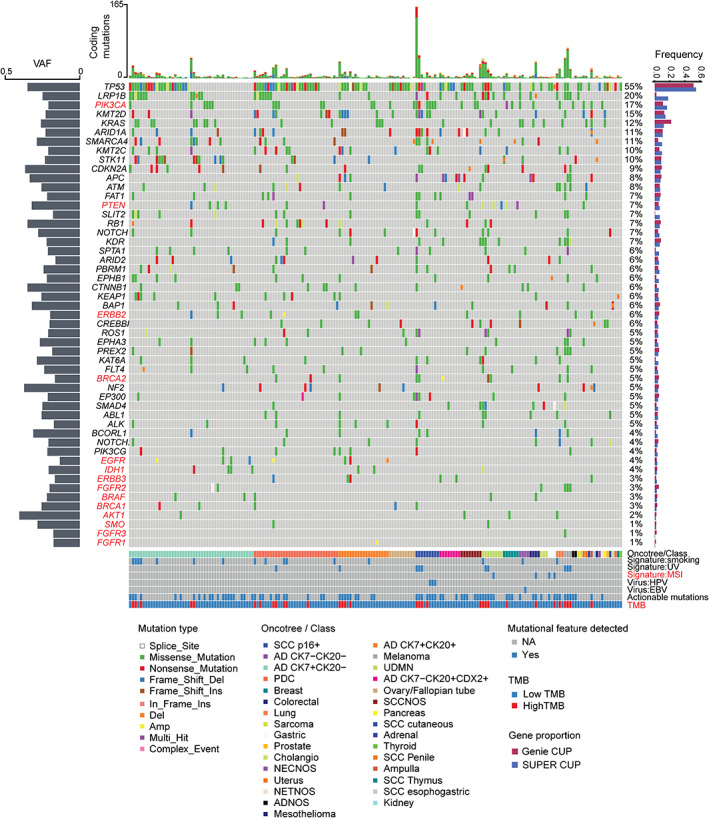
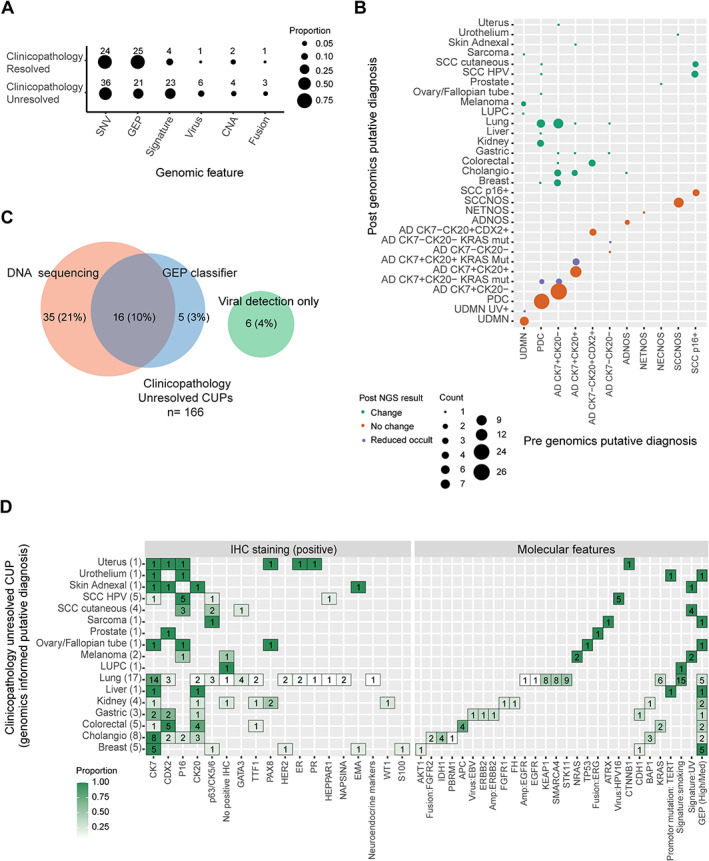
Cancer of unknown primary (CUP) is a syndrome defined by clinical absence of a primary cancer after standardised investigations. Gene expression profiling (GEP) and DNA sequencing have been used to predict primary tissue of origin (TOO) in CUP and find molecularly guided treatments; however, a detailed comparison of the diagnostic yield from these two tests has not been described. Here, we compared the diagnostic utility of RNA and DNA tests in 215 CUP patients (82% received both tests) in a prospective Australian study. Based on retrospective assessment of clinicopathological data, 77% (166/215) of CUPs had insufficient evidence to support TOO diagnosis (clinicopathology unresolved). The remainder had either a latent primary diagnosis (10%) or clinicopathological evidence to support a likely TOO diagnosis (13%) (clinicopathology resolved). We applied a microarray (CUPGuide) or custom NanoString 18-class GEP test to 191 CUPs with an accuracy of 91.5% in known metastatic cancers for high-medium confidence predictions. Classification performance was similar in clinicopathology-resolved CUPs - 80% had high-medium predictions and 94% were concordant with pathology. Notably, only 56% of the clinicopathology-unresolved CUPs had high-medium confidence GEP predictions. Diagnostic DNA features were interrogated in 201 CUP tumours guided by the cancer type specificity of mutations observed across 22 cancer types from the AACR Project GENIE database (77,058 tumours) as well as mutational signatures (e.g. smoking). Among the clinicopathology-unresolved CUPs, mutations and mutational signatures provided additional diagnostic evidence in 31% of cases. GEP classification was useful in only 13% of cases and oncoviral detection in 4%. Among CUPs where genomics informed TOO, lung and biliary cancers were the most frequently identified types, while kidney tumours were another identifiable subset. In conclusion, DNA and RNA profiling supported an unconfirmed TOO diagnosis in one-third of CUPs otherwise unresolved by clinicopathology assessment alone. DNA mutation profiling was the more diagnostically informative assay. © 2022 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of The Pathological Society of Great Britain and Ireland.
Keywords: cancer diagnostic; cancer of unknown primary; gene expression profiling; mutation profiling; targeted therapy; tissue of origin classification.
© 2022 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of The Pathological Society of Great Britain and Ireland.
Figures
References
-
- Pavlidis N, Pentheroudakis G. Cancer of unknown primary site. Lancet 2012; 379: 1428–1435. - PubMed
-
- Greco FA, Hainsworth JD. Cancer of unknown primary site. In DeVita, Hellman, and Rosenberg's Cancer: Principles and Practice of Oncology (8th edn), VT DV Jr., Hellman S, Rosenberg S (eds). Lippincott Williams & Wilkins: Philadelphia, 2008; 2363–2387.
-
- Rassy E, Pavlidis N. The currently declining incidence of cancer of unknown primary. Cancer Epidemiol 2019; 61: 139–141. - PubMed
-
- Australian Institute for Health and Welfare . Cancer data in Australia. Australian Cancer Incidence and Mortality (ACIM) books: cancer of unknown primary site. AIHW: Canberra, 2019.
-
- Massard C, Loriot Y, Fizazi K. Carcinomas of an unknown primary origin – diagnosis and treatment. Nat Rev Clin Oncol 2011; 8: 701–710. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
