

Pathophysiology Underlying Demographic and Obesity Determinants of Sleep Apnea Severity
- PMID: 36287615
- PMCID: PMC9993145
- DOI: 10.1513/AnnalsATS.202203-271OC
Pathophysiology Underlying Demographic and Obesity Determinants of Sleep Apnea Severity
Abstract
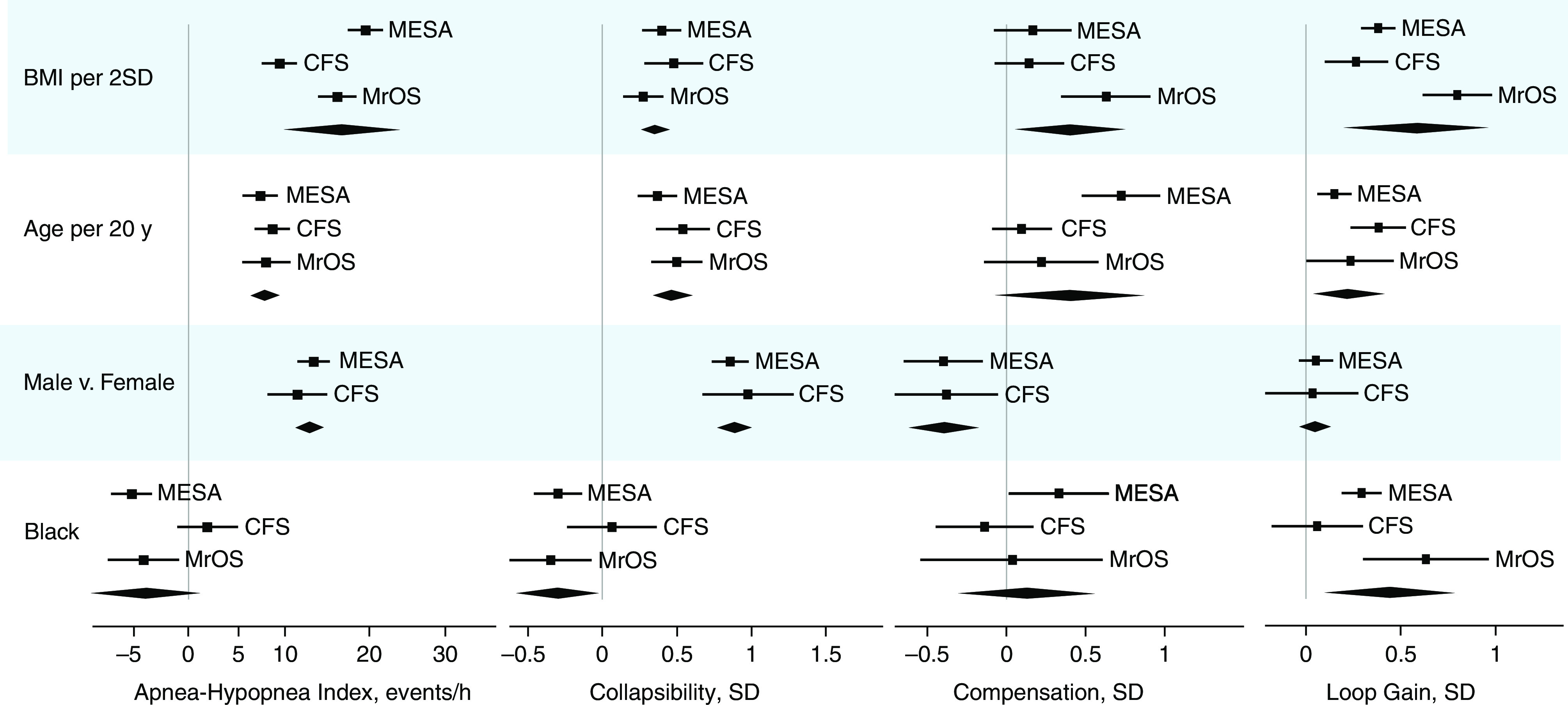
Rationale: Sleep apnea is the manifestation of key endotypic traits, including greater pharyngeal collapsibility, reduced dilator muscle compensation, and elevated chemoreflex loop gain. Objectives: We investigated how endotypic traits vary with obesity, age, sex, and race/ethnicity to influence sleep apnea disease severity (apnea-hypopnea index [AHI]). Methods: Endotypic traits were estimated from polysomnography in a diverse community-based cohort study (Multi-Ethnic Study of Atherosclerosis, N = 1,971; age range, 54-93 yr). Regression models assessed associations between each exposure (continuous variables per 2 standard deviations [SDs]) and endotypic traits (per SD) or AHI (events/h), independent of other exposures. Generalizability was assessed in two independent cohorts. Results: Greater AHI was associated with obesity (+19 events/h per 11 kg/m2 [2 SD]), male sex (+13 events/h vs. female), older age (+7 events/h per 20 yr), and Chinese ancestry (+5 events/h vs. White, obesity adjusted). Obesity-related increase in AHI was best explained by elevated collapsibility (+0.40 SD) and greater loop gain (+0.38 SD; percentage mediated, 26% [95% confidence interval (CI), 20-32%]). Male-related increase in AHI was explained by elevated collapsibility (+0.86 SD) and reduced compensation (-0.40 SD; percentage mediated, 57% [95% CI, 50-66%]). Age-related AHI increase was explained by elevated collapsibility (+0.37 SD) and greater loop gain (+0.15 SD; percentage mediated, 48% [95% CI, 34-63%]). Increased AHI with Chinese ancestry was explained by collapsibility (+0.57 SD; percentage mediated, 87% [95% CI, 57-100]). Black race was associated with reduced collapsibility (-0.30 SD) and elevated loop gain (+0.29 SD). Similar patterns were observed in the other cohorts. Conclusions: Different subgroups exhibit different underlying pathophysiological pathways to sleep apnea, highlighting the variability in mechanisms that could be targeted for intervention.
Keywords: endotype; epidemiology; pathophysiology; precision medicine.
Figures

References
Publication types
MeSH terms
Grants and funding
- R01HL098433/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- R01HL070837/HL/NHLBI NIH HHS/United States
- R01 HL071194/HL/NHLBI NIH HHS/United States
- R01HL070838/HL/NHLBI NIH HHS/United States
- K23 HL159259/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- R01 HL070839/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- R01 HL070837/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- R01 HL070848/HL/NHLBI NIH HHS/United States
- R01 HL046380/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- UL1TR001079/TR/NCATS NIH HHS/United States
- R01 HL070847/HL/NHLBI NIH HHS/United States
- R01HL071194/HL/NHLBI NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- R01HL070841/HL/NHLBI NIH HHS/United States
- T32HL07567/NH/NIH HHS/United States
- R01 HL070842/HL/NHLBI NIH HHS/United States
- R01HL070839/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- R35HL135818/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R35 HL135818/HL/NHLBI NIH HHS/United States
- R01 HL098433/HL/NHLBI NIH HHS/United States
- R01HL146697/HL/NHLBI NIH HHS/United States
- R01HL070842/HL/NHLBI NIH HHS/United States
- R24HL114473/NH/NIH HHS/United States
- R01 HL070841/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- R01 HL070838/HL/NHLBI NIH HHS/United States
- R01HL070848/HL/NHLBI NIH HHS/United States
- UL1TR001420/TR/NCATS NIH HHS/United States
- R24 HL114473/HL/NHLBI NIH HHS/United States
- NH/NIH HHS/United States
- UL1TR000040/TR/NCATS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- R01HL070847/HL/NHLBI NIH HHS/United States
- T32 HL007567/HL/NHLBI NIH HHS/United States
- R01 HL146697/HL/NHLBI NIH HHS/United States
- R01HL046380/NH/NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- L30 HL143623/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
