

Radiation Dose Reduction Opportunities in Vascular Imaging
- PMID: 36287818
- PMCID: PMC9607049
- DOI: 10.3390/tomography8050219
Radiation Dose Reduction Opportunities in Vascular Imaging
Abstract
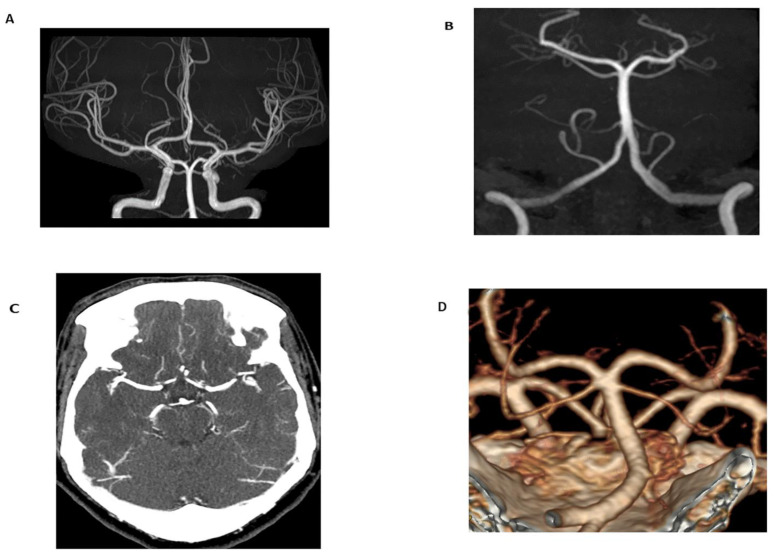
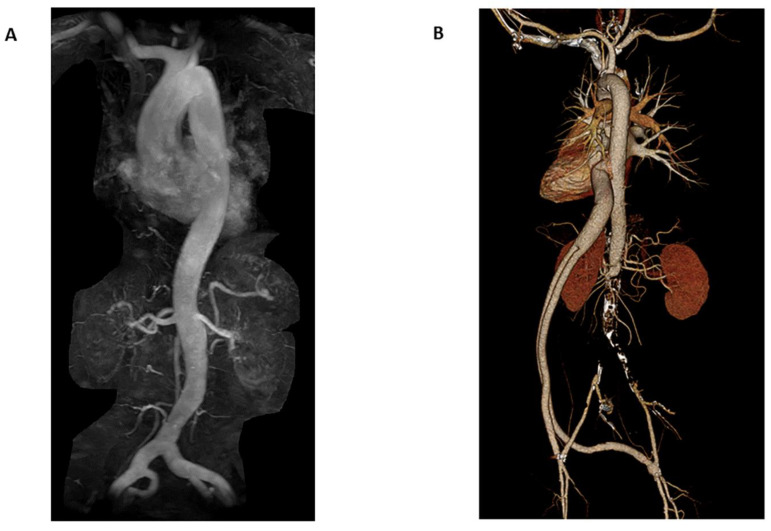
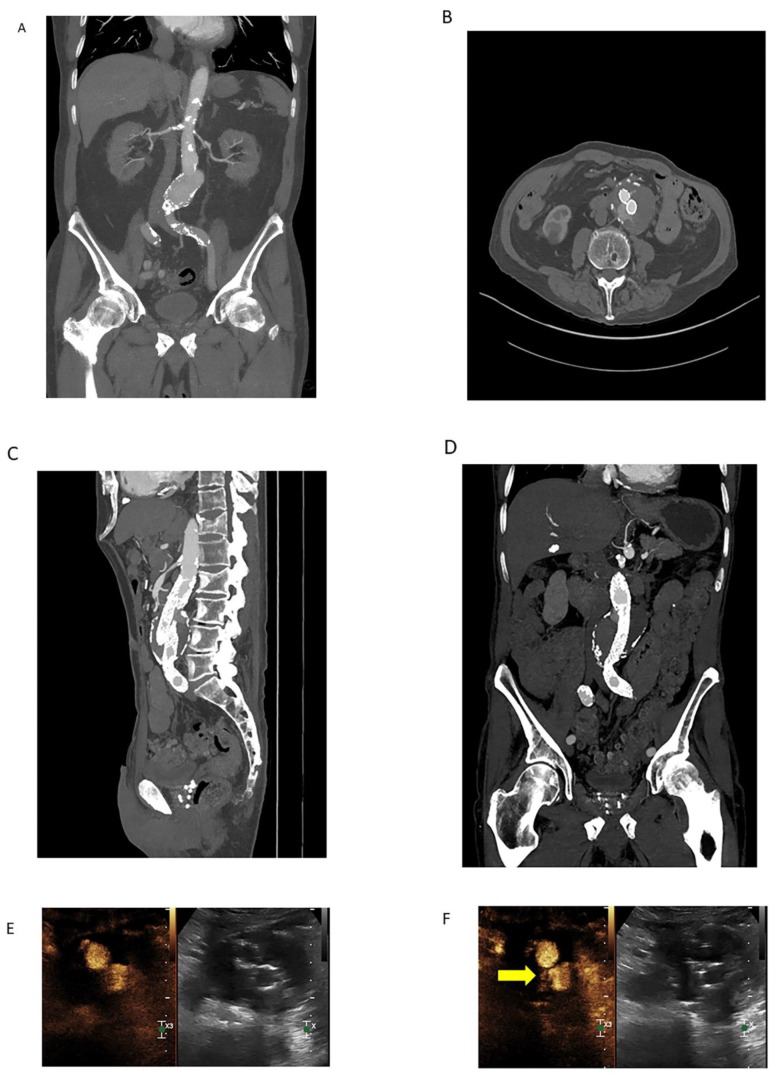
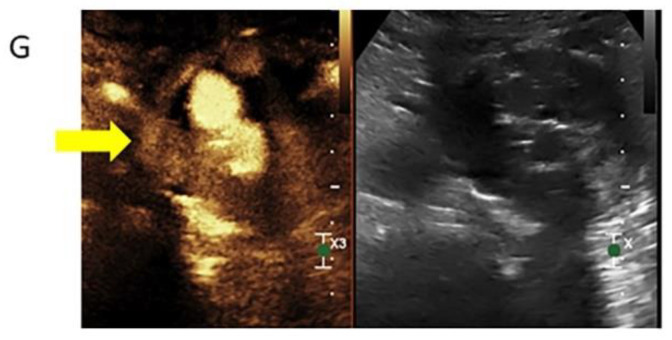
Computed tomography angiography (CTA) has been the gold standard imaging modality for vascular imaging due to a variety of factors, including the widespread availability of computed tomography (CT) scanners, the ease and speed of image acquisition, and the high sensitivity of CTA for vascular pathology. However, the radiation dose experienced by the patient during imaging has long been a concern of this image acquisition method. Advancements in CT image acquisition techniques in combination with advancements in non-ionizing radiation imaging techniques including magnetic resonance angiography (MRA) and contrast-enhanced ultrasound (CEUS) present growing opportunities to reduce total radiation dose to patients. This review provides an overview of advancements in imaging technology and acquisition techniques that are helping to minimize radiation dose associated with vascular imaging.
Keywords: computed tomography angiography; magnetic resonance angiography; radiation dose; radiation reduction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- National Research Council, Division on Earth and Life Studies, Board on Radiation Effects Research, Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation . Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2. National Academies Press; Washington, DC, USA: 2006.
-
- AAPM Position Statements, Policies and Procedures—Details 2018. [(accessed on 6 August 2022)]. Available online: https://www.aapm.org/org/policies/details.asp?type=PP&id=2548.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
