

Clonal IgA and IgG autoantibodies from individuals at risk for rheumatoid arthritis identify an arthritogenic strain of Subdoligranulum
- PMID: 36288282
- PMCID: PMC9804515
- DOI: 10.1126/scitranslmed.abn5166
Clonal IgA and IgG autoantibodies from individuals at risk for rheumatoid arthritis identify an arthritogenic strain of Subdoligranulum
Abstract
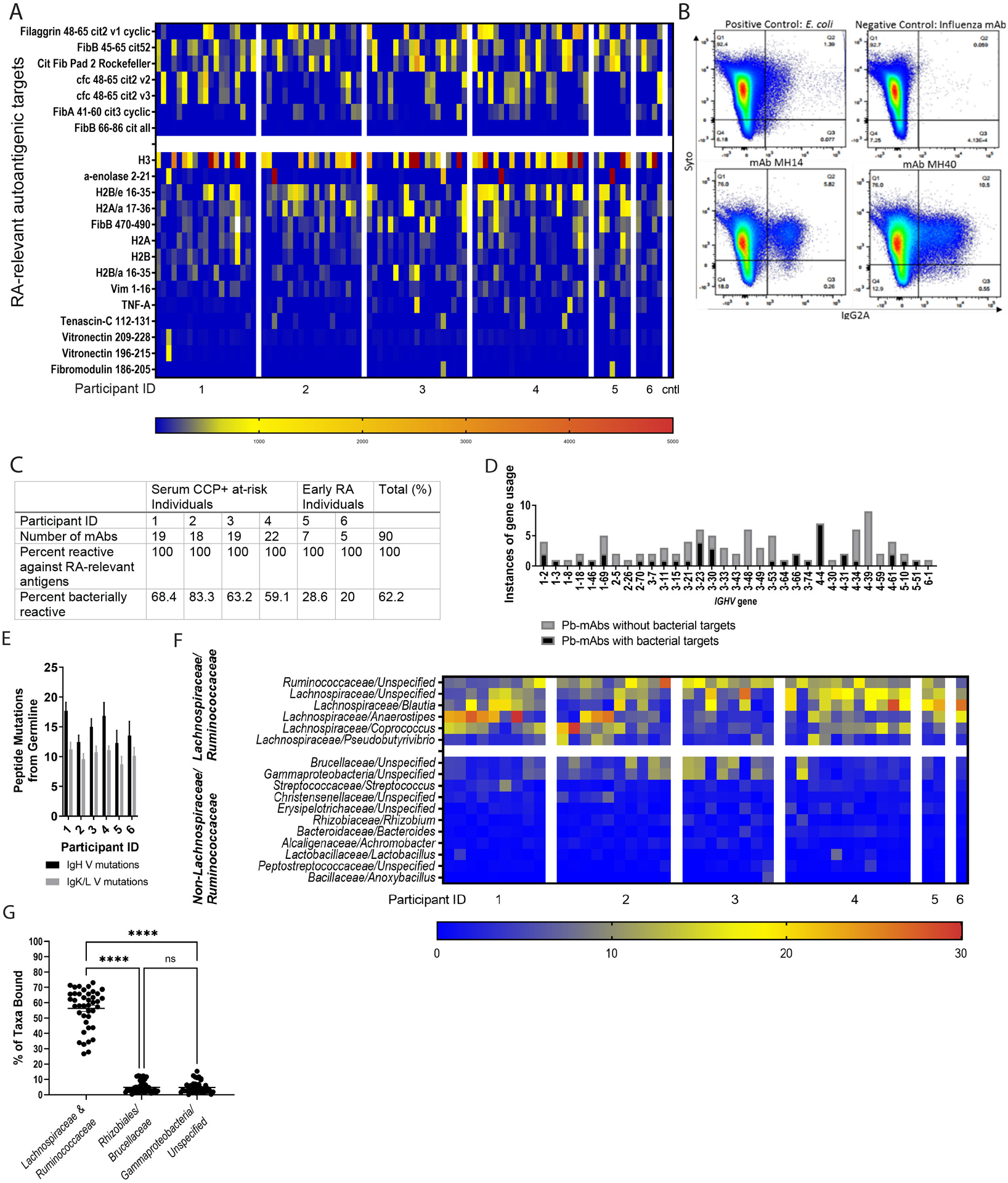
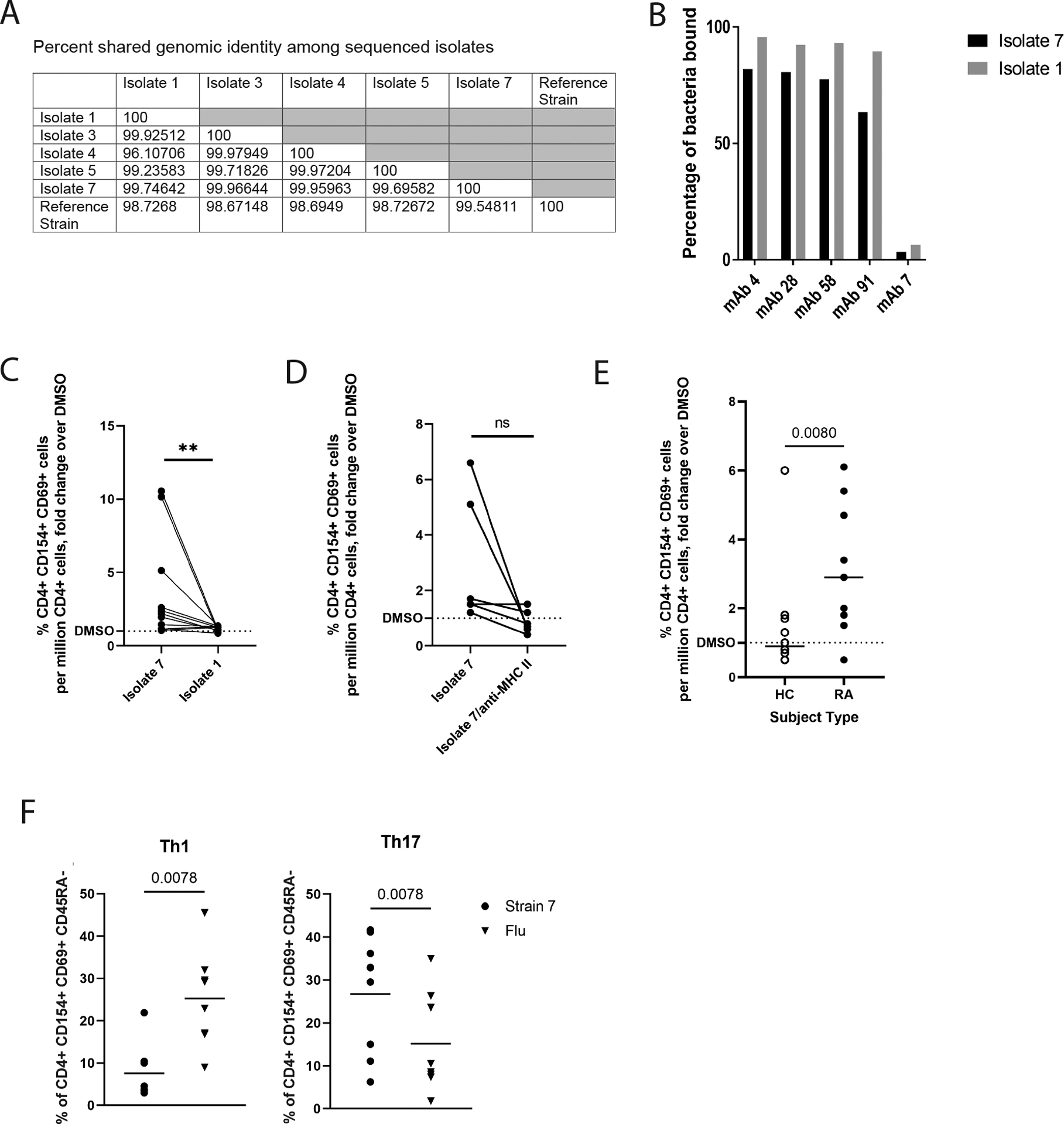
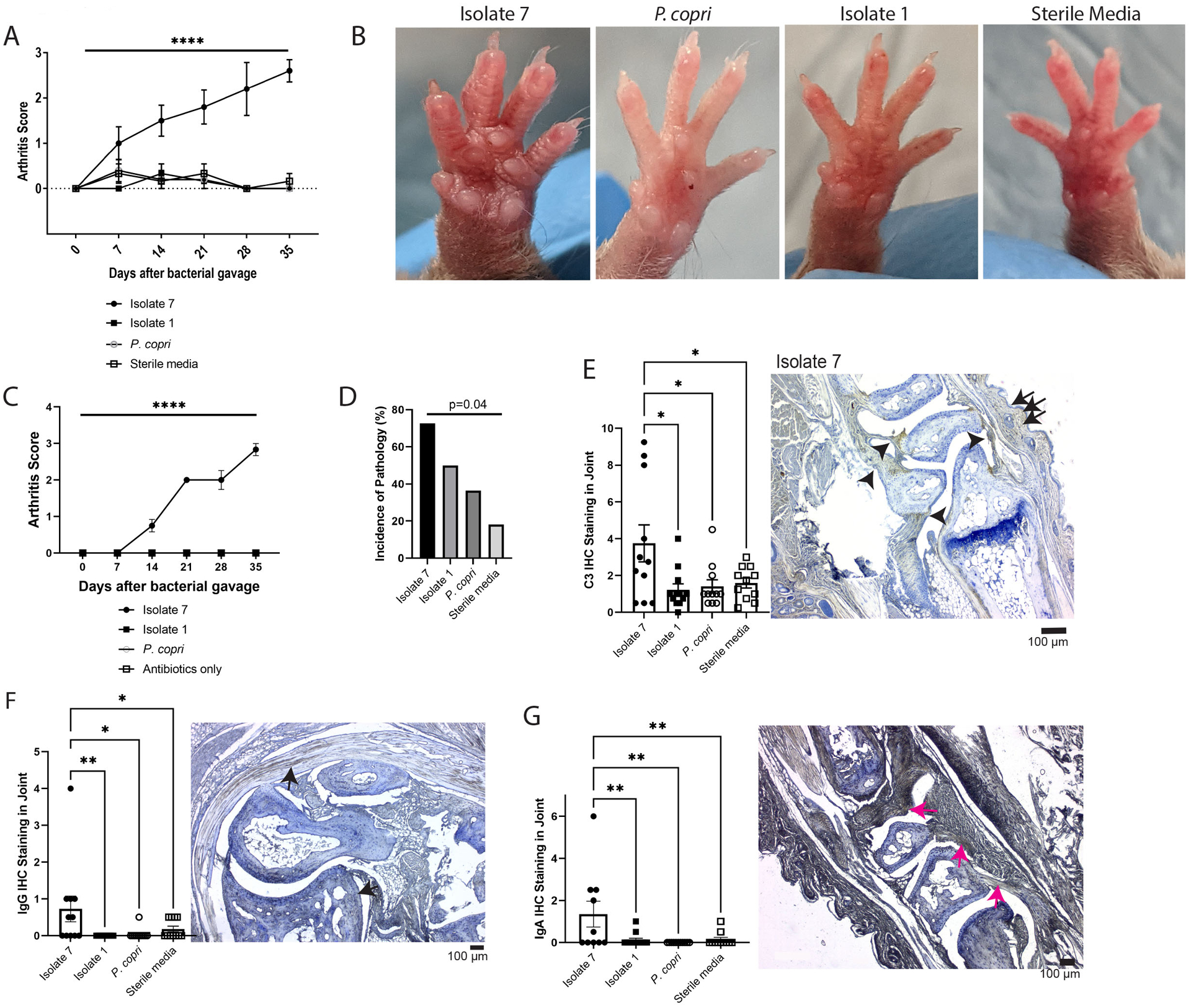
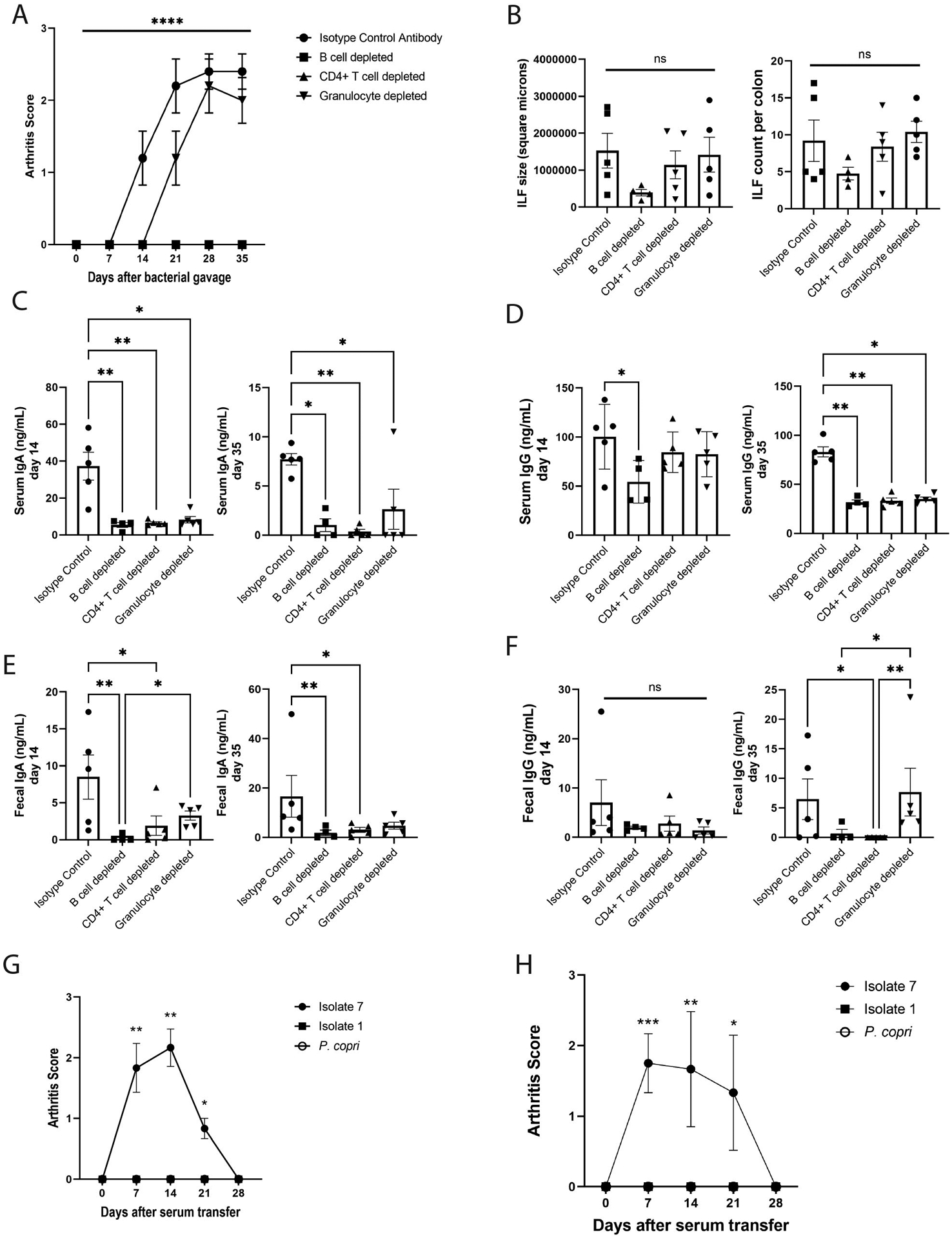
The mucosal origins hypothesis of rheumatoid arthritis (RA) proposes a central role for mucosal immune responses in the initiation or perpetuation of the systemic autoimmunity that occurs with disease. However, the connection between the mucosa and systemic autoimmunity in RA remains unclear. Using dual immunoglobulin A (IgA) and IgG family plasmablast-derived monoclonal autoantibodies obtained from peripheral blood of individuals at risk for RA, we identified cross-reactivity between RA-relevant autoantigens and bacterial taxa in the closely related families Lachnospiraceae and Ruminococcaceae. After generating bacterial isolates within the Lachnospiraceae/Ruminococcaceae genus Subdoligranulum from the feces of an individual, we confirmed monoclonal antibody binding and CD4+ T cell activation in individuals with RA compared to control individuals. In addition, when Subdoligranulum isolate 7 but not isolate 1 colonized germ-free mice, it stimulated TH17 cell expansion, serum RA-relevant IgG autoantibodies, and joint swelling reminiscent of early RA, with histopathology characterized by antibody deposition and complement activation. Systemic immune responses were likely due to mucosal invasion along with the generation of colon-isolated lymphoid follicles driving increased fecal and serum IgA by isolate 7, because B and CD4+ T cell depletion not only halted intestinal immune responses but also eliminated detectable clinical disease. In aggregate, these findings demonstrate a mechanism of RA pathogenesis through which a specific intestinal strain of bacteria can drive systemic autoantibody generation and joint-centered antibody deposition and immune activation.
Conflict of interest statement
Competing Interests: The authors have no conflicts of interests to declare.
Figures


Comment in
-
Pre-RA autoantibodies recognize arthritogenic gut bacterium.Nat Rev Rheumatol. 2023 Jan;19(1):1. doi: 10.1038/s41584-022-00884-3. Nat Rev Rheumatol. 2023. PMID: 36446917 No abstract available.
-
Fishing with autoantibodies nets a gut bacteria that drives arthritis.Sci Immunol. 2022 Dec 9;7(78):eadf9316. doi: 10.1126/sciimmunol.adf9316. Epub 2022 Dec 2. Sci Immunol. 2022. PMID: 36459567
-
Subdoligranulum chews up joints: how a gut pathobiont can instigate arthritis.Trends Immunol. 2023 Jan;44(1):4-6. doi: 10.1016/j.it.2022.11.006. Epub 2022 Dec 6. Trends Immunol. 2023. PMID: 36494272
-
The bacterial link with rheumatoid arthritis.Int J Rheum Dis. 2023 Apr;26(4):603-604. doi: 10.1111/1756-185X.14598. Int J Rheum Dis. 2023. PMID: 37002901 No abstract available.
References
-
- Nielen MM, van Schaardenburg D, Reesink HW, van de Stadt RJ, van der Horst-Bruinsma IE, de Koning MH, Habibuw MR, Vandenbroucke JP, Dijkmans BA, Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum 50, 380386 (2004); published online Epub Feb (10.1002/art.20018). - DOI - PubMed
-
- Arlestig L, Mullazehi M, Kokkonen H, Rocklov J, Ronnelid J, Dahlqvist SR, Antibodies against cyclic citrullinated peptides of IgG, IgA and IgM isotype and rheumatoid factor of IgM and IgA isotype are increased in unaffected members of multicase rheumatoid arthritis families from northern Sweden. Ann Rheum Dis 71, 825–829 (2012); published online Epub Jun (10.1136/annrheumdis-2011-200668). - DOI - PMC - PubMed
-
- Sokolove J, Bromberg R, Deane KD, Lahey LJ, Derber LA, Chandra PE, Edison JD, Gilliland WR, Tibshirani RJ, Norris JM, Holers VM, Robinson WH, Autoantibody epitope spreading in the pre-clinical phase predicts progression to rheumatoid arthritis. PLoS One 7, e35296 (2012)10.1371/journal.pone.0035296). - DOI - PMC - PubMed
-
- Kelmenson LB, Wagner BD, McNair BK, Frazer-Abel A, Demoruelle MK, Bergstedt DT, Feser ML, Moss LK, Parish MC, Mewshaw EA, Mikuls TR, Edison JD, Holers VM, Deane KD, Timing of Elevations of Autoantibody Isotypes Prior to Diagnosis of Rheumatoid Arthritis. Arthritis Rheumatol 72, 251–261 (2020); published online Epub Feb (10.1002/art.41091). - DOI - PMC - PubMed
-
- Gerlag DM, Raza K, van Baarsen LG, Brouwer E, Buckley CD, Burmester GR, Gabay C, Catrina AI, Cope AP, Cornelis F, Dahlqvist SR, Emery P, Eyre S, Finckh A, Gay S, Hazes JM, van der Helm-van Mil A, Huizinga TW, Klareskog L, Kvien TK, Lewis C, Machold KP, Ronnelid J, van Schaardenburg D, Schett G, Smolen JS, Thomas S, Worthington J, Tak PP, EULAR recommendations for terminology and research in individuals at risk of rheumatoid arthritis: report from the Study Group for Risk Factors for Rheumatoid Arthritis. Ann Rheum Dis 71, 6382013641 (2012); published online Epub May (10.1136/annrheumdis-2011-200990). - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
