

Association between coronary artery calcium and all-cause mortality: A large single-center retrospective cohort study
- PMID: 36288331
- PMCID: PMC9604986
- DOI: 10.1371/journal.pone.0276659
Association between coronary artery calcium and all-cause mortality: A large single-center retrospective cohort study
Abstract
Objective: Previous studies have revealed that coronary artery calcium is related to cardiovascular diseases and mortality. However, most studies have been conducted in Western countries and have excluded patients with pre-existing heart disease. We investigated the association between coronary artery calcium (CAC) and all-cause mortality in an Asian cohort and in subgroups stratified by age, sex, smoking, obesity, diabetes, cardiovascular disease, blood pressure, and biochemical parameters.
Methods: We conducted a retrospective cohort study on 4529 health examinees who underwent multidetector computed tomography in a tertiary medical center in Taiwan between 2011 and 2016. The mean follow-up was 3.5 years. Cox regression was used to estimate the relative hazards of death. Stratified analyses were performed.
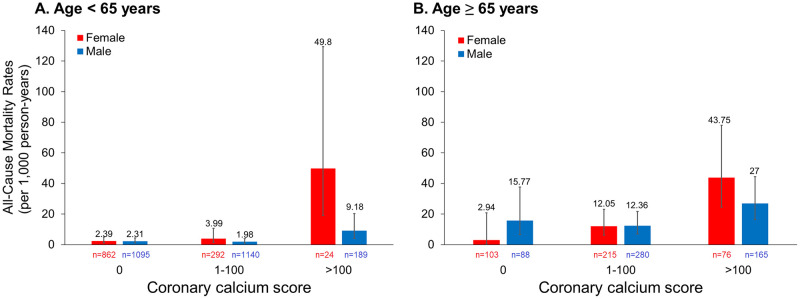
Results: The all-cause mortality rates were 2.94, 4.88, 17.6, and 33.1 per 1000 person-years for CAC scores of 0, 1-100, 101-400, and >400, respectively. The multivariable adjusted hazard ratios (95% confidence intervals [CIs]) for all-cause mortality were 0.95 (0.53, 1.72), 1.87 (0.89, 3.90), and 3.05 (1.46, 6.39) for CAC scores of 1-100, 101-400, and >400, respectively, relative to a CAC score of 0. Compared with CAC ≤ 400, the HRs (95% CIs) for CAC > 400 were 6.46 (2.44, 17.15) and 1.94 (1.00, 3.76) in younger and older adults, respectively, indicating that age was a moderating variable (p = 0.02).
Conclusion: High CAC scores were associated with increased all-cause mortality. Although older adult patients had higher risks of death, the relative risk of death for patients with CAC > 400 was more prominent in people younger than 65 years.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Antikainen R, Jousilahti P, Tuomilehto J. Systolic blood pressure, isolated systolic hypertension and risk of coronary heart disease, strokes, cardiovascular disease and all-cause mortality in the middle-aged population. Journal of Hypertension. 1998;16(5):577–83. doi: 10.1097/00004872-199816050-00004 - DOI - PubMed
-
- Wei M, Mitchell BD, Haffner SM, Stem MP. Effects of cigarette smoking, diabetes, high cholesterol, and hypertension on all-cause mortality and cardiovascular disease mortality in Mexican Americans: the San Antonio Heart Study. American Journal of Epidemiology. 1996;144(11):1058–65. - PubMed
-
- Wei M, Gaskill SP, Haffner SM, Stern MP. Effects of diabetes and level of glycemia on all-cause and cardiovascular mortality: the San Antonio Heart Study. Diabetes Care. 1998;21(7):1167–72. - PubMed
-
- Okamura T, Tanaka H, Miyamatsu N, Hayakawa T, Kadowaki T, Kita Y, et al.. The relationship between serum total cholesterol and all-cause or cause-specific mortality in a 17.3-year study of a Japanese cohort. Atherosclerosis. 2007;190(1):216–23. doi: 10.1016/j.atherosclerosis.2006.01.024 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
