

Neoadjuvant relatlimab and nivolumab in resectable melanoma
- PMID: 36289334
- PMCID: PMC9607737
- DOI: 10.1038/s41586-022-05368-8
Neoadjuvant relatlimab and nivolumab in resectable melanoma
Erratum in
-
Author Correction: Neoadjuvant relatlimab and nivolumab in resectable melanoma.Nature. 2023 Mar;615(7953):E23. doi: 10.1038/s41586-023-05892-1. Nature. 2023. PMID: 36894629 Free PMC article. No abstract available.
Abstract
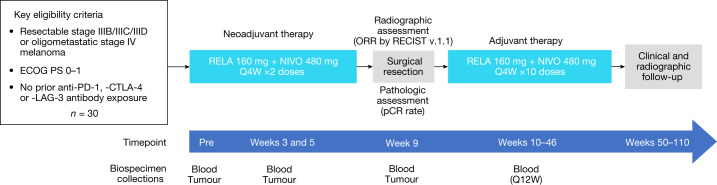
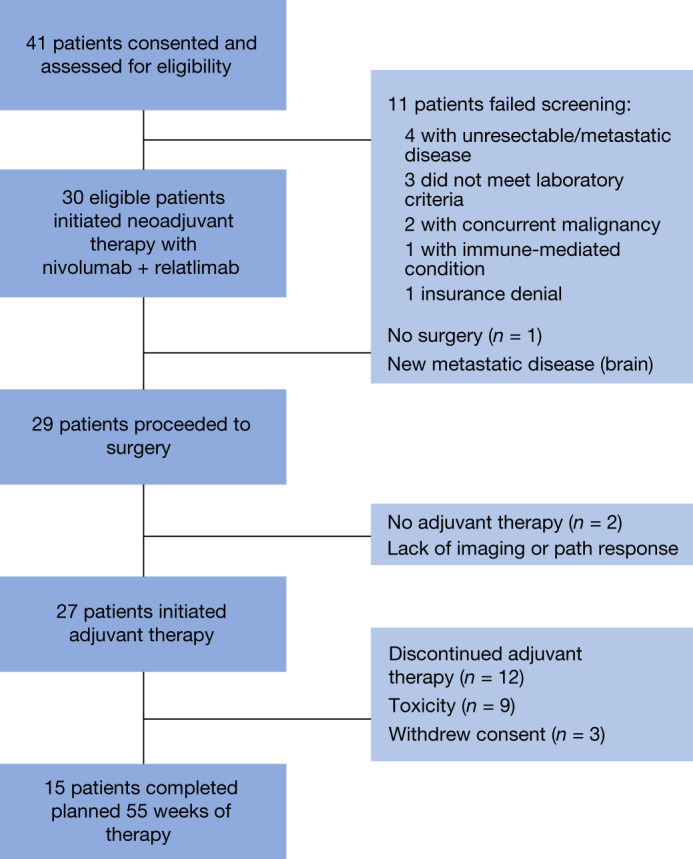
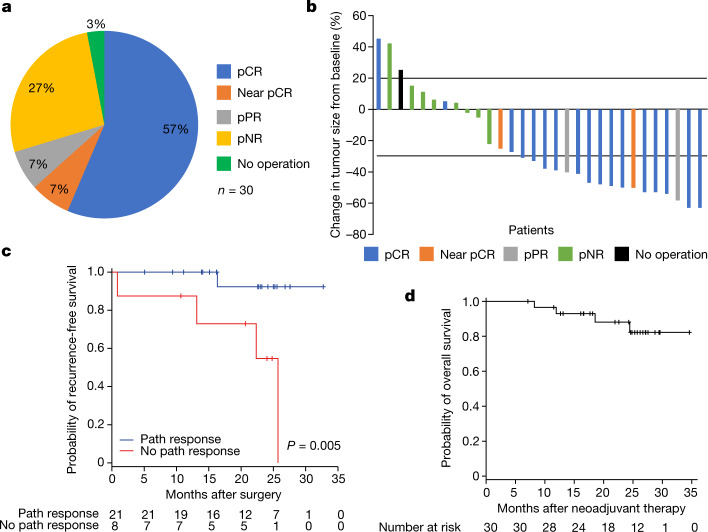
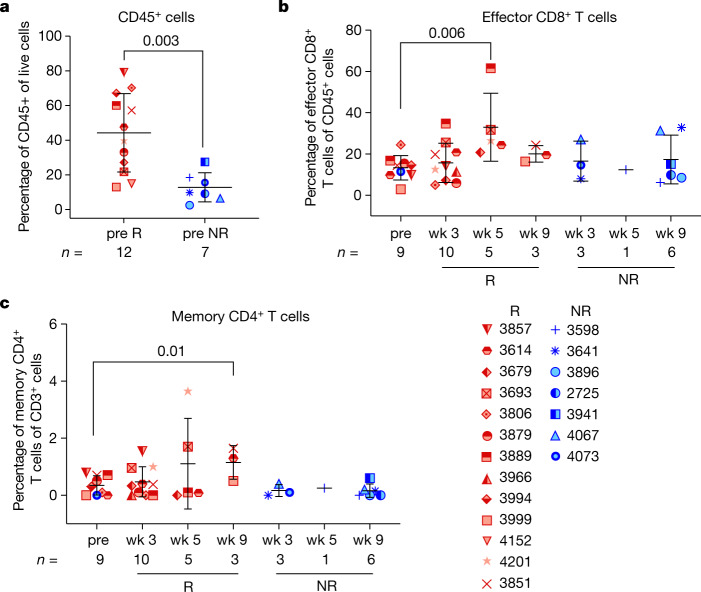
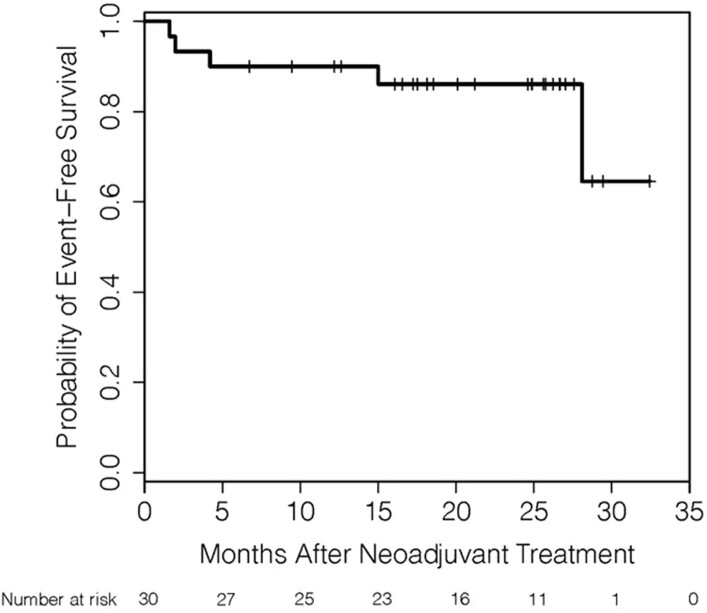
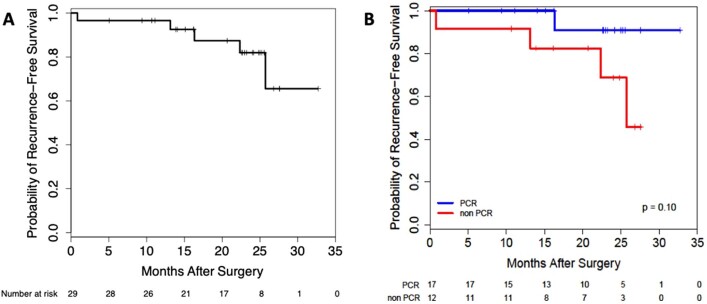
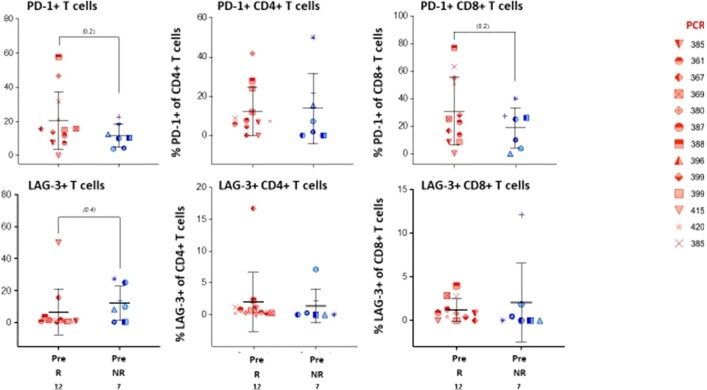
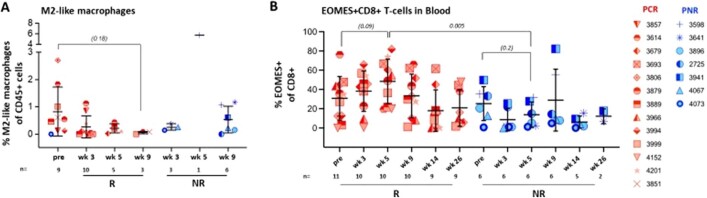
Relatlimab and nivolumab combination immunotherapy improves progression-free survival over nivolumab monotherapy in patients with unresectable advanced melanoma1. We investigated this regimen in patients with resectable clinical stage III or oligometastatic stage IV melanoma (NCT02519322). Patients received two neoadjuvant doses (nivolumab 480 mg and relatlimab 160 mg intravenously every 4 weeks) followed by surgery, and then ten doses of adjuvant combination therapy. The primary end point was pathologic complete response (pCR) rate2. The combination resulted in 57% pCR rate and 70% overall pathologic response rate among 30 patients treated. The radiographic response rate using Response Evaluation Criteria in Solid Tumors 1.1 was 57%. No grade 3-4 immune-related adverse events were observed in the neoadjuvant setting. The 1- and 2-year recurrence-free survival rate was 100% and 92% for patients with any pathologic response, compared to 88% and 55% for patients who did not have a pathologic response (P = 0.005). Increased immune cell infiltration at baseline, and decrease in M2 macrophages during treatment, were associated with pathologic response. Our results indicate that neoadjuvant relatlimab and nivolumab induces a high pCR rate. Safety during neoadjuvant therapy is favourable compared to other combination immunotherapy regimens. These data, in combination with the results of the RELATIVITY-047 trial1, provide further confirmation of the efficacy and safety of this new immunotherapy regimen.
© 2022. The Author(s).
Conflict of interest statement
R.N.A.: research funding from Bristol-Myers Squibb, Iovance, Merck and Novartis; consulting role for Bristol-Myers Squibb, Iovance and Novartis. M. Postow: consulting fees from Aduro, Array BioPharma, Bristol-Myers Squibb, Eisai, Incyte, Merck, NewLink Genetics, Novartis and Pfizer; honoraria from Bristol-Myers Squibb and Merck; institutional support from Array BioPharma, AstraZeneca, Bristol-Myers Squibb, Infinity, Merck, Novartis and RGenix. M.I.R.: clinical research funding from Amgen; consulting/advisory board member role for Amgen, Castle BioSciences, Merck and Novartis. I.C.G.: research funding from Bristol-Myers Squibb, Merck and Pfizer; consulting role for Bristol-Myers Squibb and Novartis. J.L.M.: honoraria for Bristol-Myers Squibb and Roche; consultant for Merck. M.K.W.: advisory boards for Adagene, Bristol-Myers Squibb, Castle Biosciences, EMD-Serono, ExiCure, Merck, Pfizer and Regeneron. J.E.G.: consultant and/or advisory role; Merck and Regeneron. A.N.S.: research funding from Bristol-Myers Squibb, Checkmate Pharmaceuticals, Foghorn Therapeutics, Immunocore, Novartis, Pfizer, Polaris, Targovax and Xcovery; advisory board for Bristol-Myers Squibb, Immunocore and Novartis. A.D.: research funding from Apexigen, Idera and Nektar; consulting for Apexigen, Idera, Memgen, Nektar and Pfizer. S.P.P.: research funding from Bristol-Myers Squibb, Ideaya and Provectus; consulting honoraria from Cardinal Health, Castle Biosciences and Merck. M.A.D.: consultant to ABM Therapeutics, Apexigen, Array, Bristol-Myers Squibb, Eisai, GlaxoSmithKline, Pfizer, Roche/Genentech, Novartis, Sanofi-Aventis and Vaccinex; PI of research grants to GlaxoSmithKline, MD Anderson by Roche/Genentech, Merck, Myriad, Oncothyreon and Sanofi-Aventis. J.P.A.: consulting or stock ownership or advisory board for Achelois, Adaptive Biotechnologies, Apricity, BioAtla, BioNTech, Candel Therapeutics, Codiak, Dragonfly, Earli, Enable Medicine, Hummingbird, ImaginAb, Jounce, Lava Therapeutics, Lytix, Marker, PBM Capital, Phenomic AI, Polaris Pharma, Time Bioventures, Trained Therapeutix and Venn Biosciences. P.S.: consulting or stock ownership or advisory board for Achelois, Adaptive Biotechnologies, Affini-T, Apricity, BioAtla, BioNTech, Candel Therapeutics, Catalio, Codiak, Constellation, Dragonfly, Earli, Enable Medicine, Glympse, Hummingbird, ImaginAb, Infinity Pharma, Jounce, JSL Health, Lava Therapeutics, Lytix, Marker, MedImmune, Oncolytics, PBM Capital, Phenomic AI, Polaris Pharma, Sporos, Time Bioventures, Trained Therapeutix and Venn Biosciences. J.A.W.: compensation for speaker’s bureau and honoraria from Bristol-Myers Squibb, Dava Oncology, Gilead, Illumina, Imedex, MedImmune, Omniprex, PeerView and Physician Education Resource; consultant/advisory board member for AstraZeneca, Biothera Pharmaceuticals, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Micronoma, Novartis and Roche/Genentech. C.A.: consulting fees from Iovance. H.A.T.: research funding from GlaxoSmithKline; research funding and consulting honoraria from Bristol-Myers Squibb, Genentech, Merck and Novartis; consulting for Boxer, Eisai, Iovance, Karyopharm and Pfizer. All other authors report no conflicts of interest.
Figures
Comment in
-
Relatlimab and nivolumab in the treatment of melanoma.Cell. 2022 Dec 22;185(26):4866-4869. doi: 10.1016/j.cell.2022.12.003. Cell. 2022. PMID: 36563660
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
