

An explainable model of host genetic interactions linked to COVID-19 severity
- PMID: 36289370
- PMCID: PMC9606365
- DOI: 10.1038/s42003-022-04073-6
An explainable model of host genetic interactions linked to COVID-19 severity
Abstract
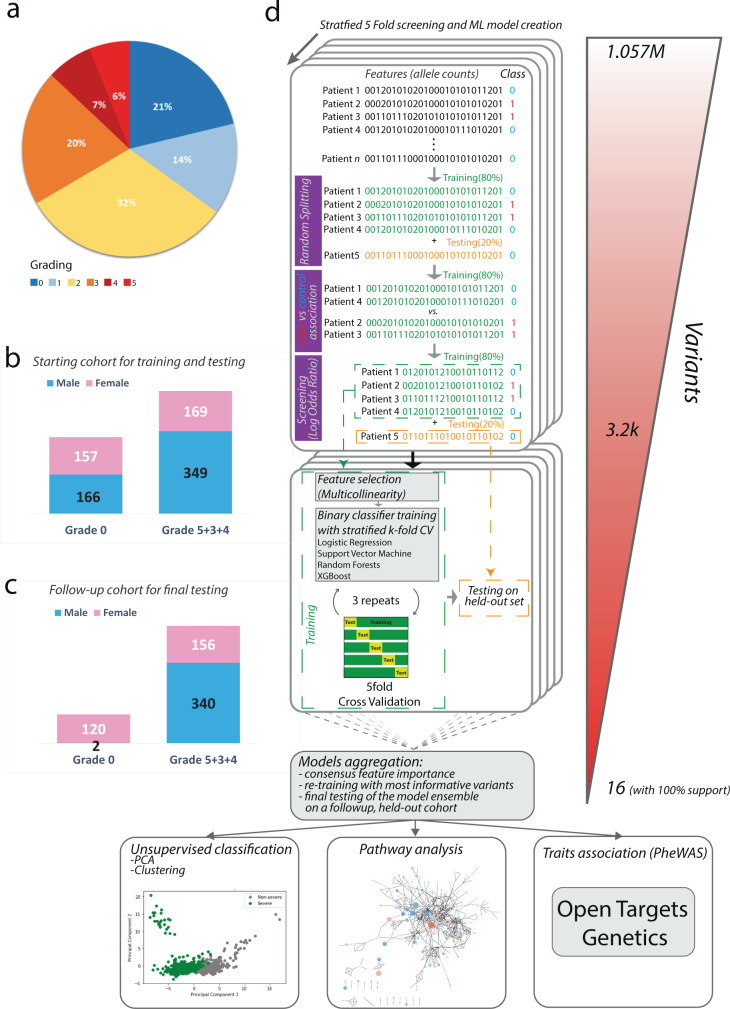
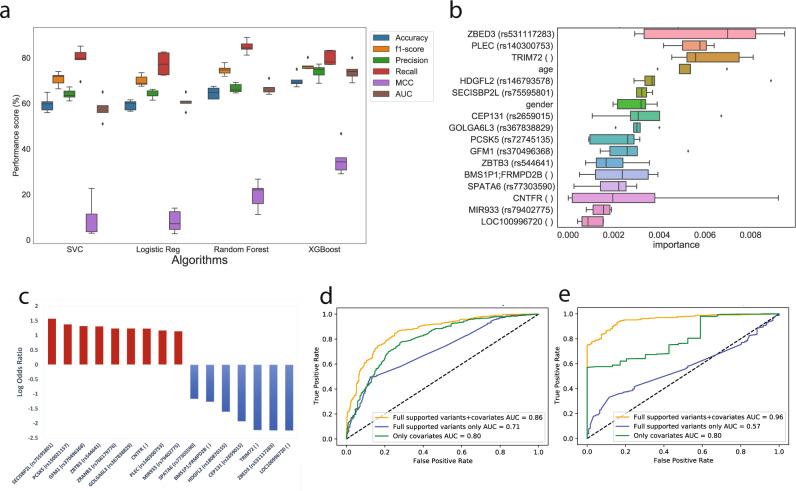
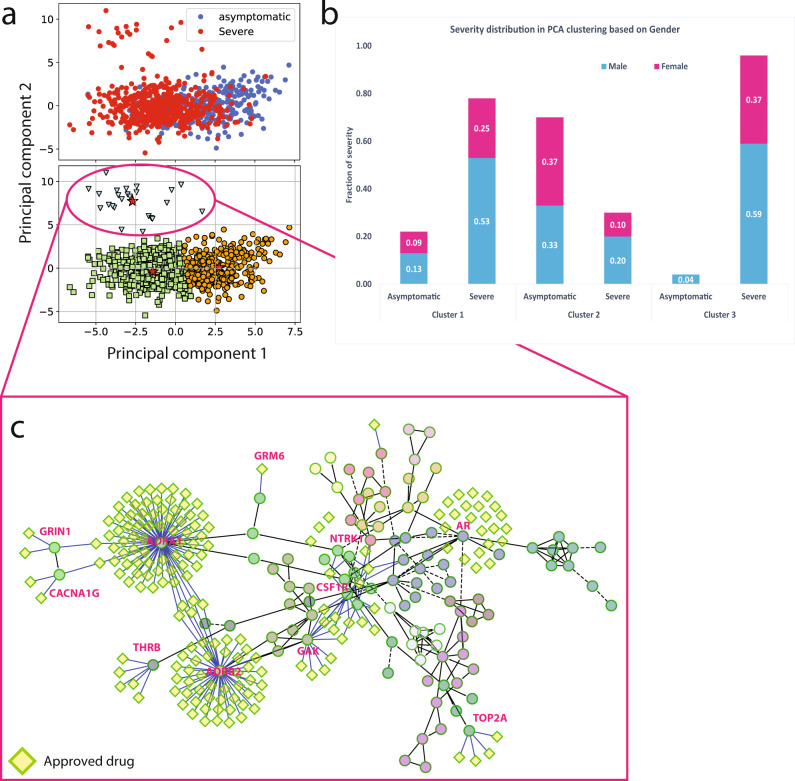
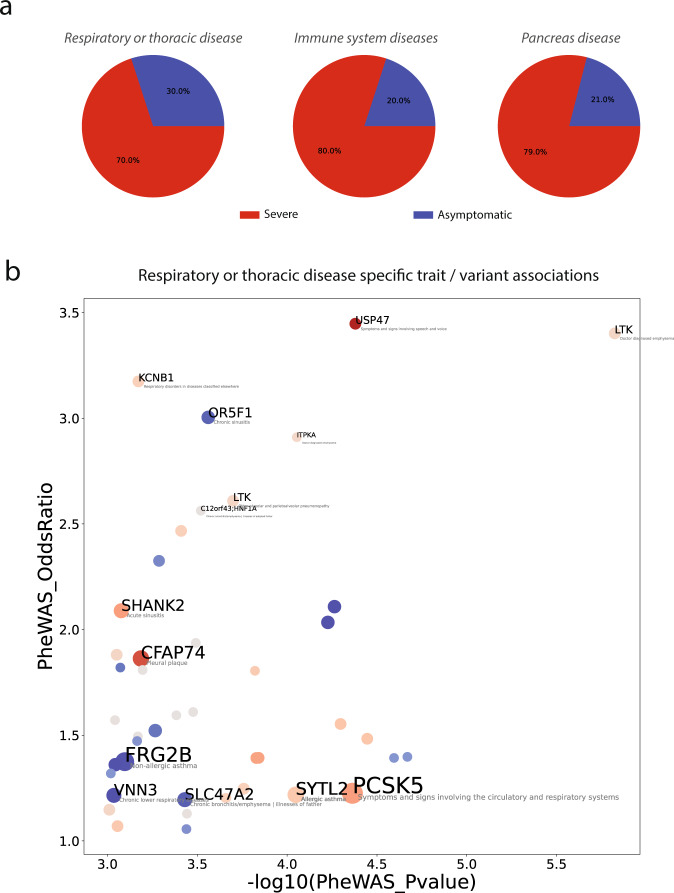
We employed a multifaceted computational strategy to identify the genetic factors contributing to increased risk of severe COVID-19 infection from a Whole Exome Sequencing (WES) dataset of a cohort of 2000 Italian patients. We coupled a stratified k-fold screening, to rank variants more associated with severity, with the training of multiple supervised classifiers, to predict severity based on screened features. Feature importance analysis from tree-based models allowed us to identify 16 variants with the highest support which, together with age and gender covariates, were found to be most predictive of COVID-19 severity. When tested on a follow-up cohort, our ensemble of models predicted severity with high accuracy (ACC = 81.88%; AUCROC = 96%; MCC = 61.55%). Our model recapitulated a vast literature of emerging molecular mechanisms and genetic factors linked to COVID-19 response and extends previous landmark Genome-Wide Association Studies (GWAS). It revealed a network of interplaying genetic signatures converging on established immune system and inflammatory processes linked to viral infection response. It also identified additional processes cross-talking with immune pathways, such as GPCR signaling, which might offer additional opportunities for therapeutic intervention and patient stratification. Publicly available PheWAS datasets revealed that several variants were significantly associated with phenotypic traits such as "Respiratory or thoracic disease", supporting their link with COVID-19 severity outcome.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bastard P, et al. IgG autoantibodies against type I IFNs in patients with severe COVID-19. Sci. (80-.). 2020;4585:1–19.
