

Can passive leg raise predict the response to fluid resuscitation in ED?
- PMID: 36289475
- PMCID: PMC9608892
- DOI: 10.1186/s12873-022-00721-6
Can passive leg raise predict the response to fluid resuscitation in ED?
Abstract
Objective: Passive leg raise (PLR) can be used as a reversible preload challenge to stratify patients according to preload response. We aim to evaluate the accuracy of PLR, monitored by a non-invasive cardiac output monitor in predicting to response to fluid resuscitation in emergency department (ED).
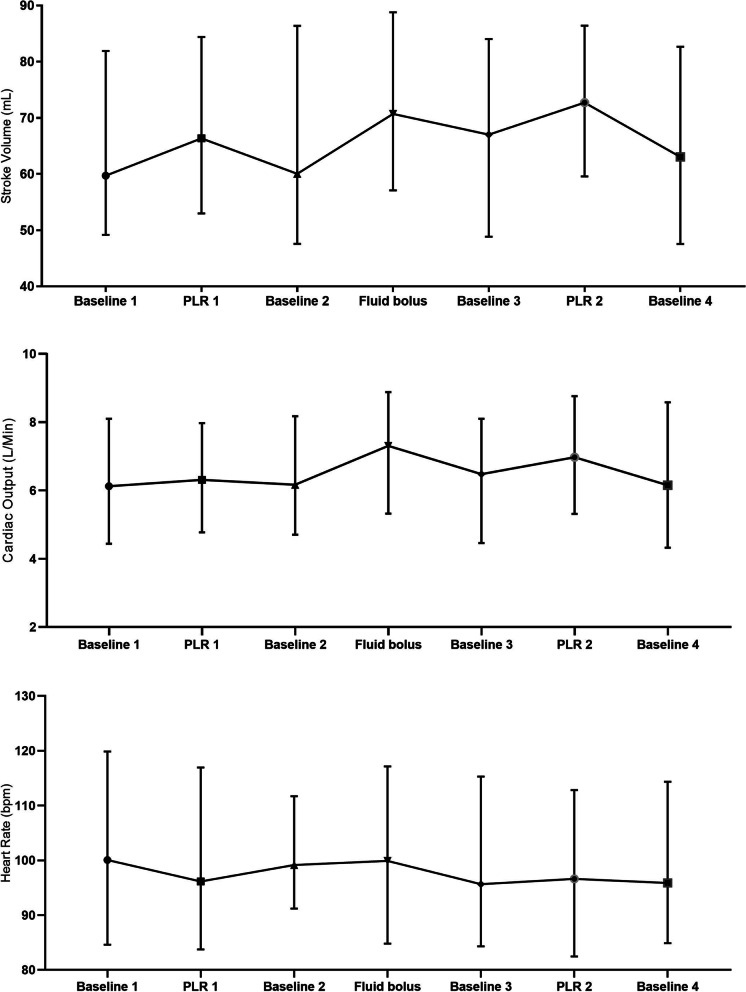
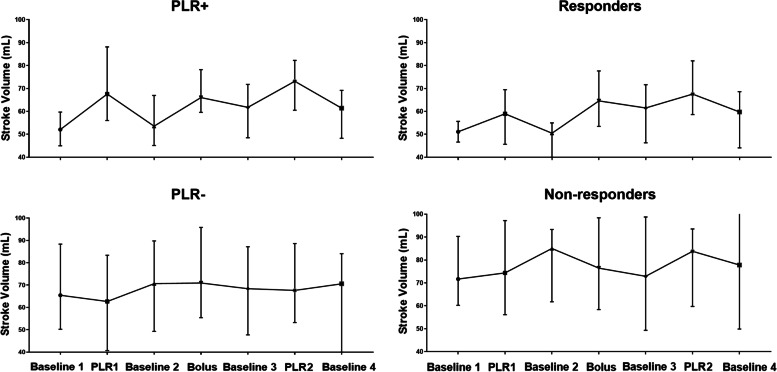
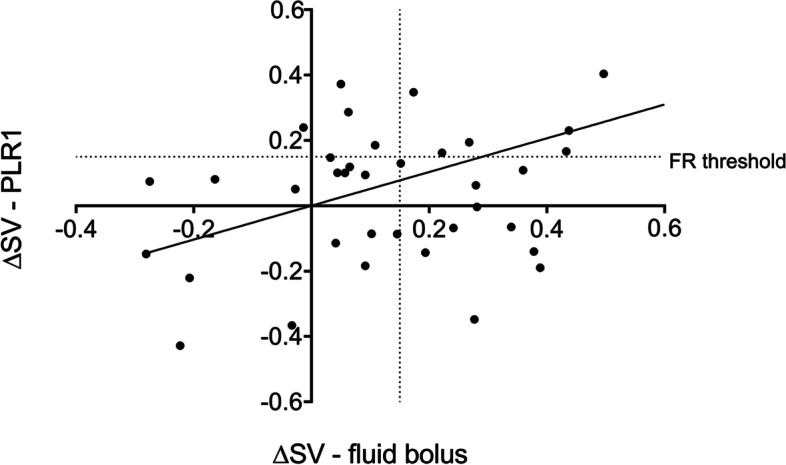
Methods: We recruited adult patients planned to receive a resuscitation fluid bolus. Patients were monitored using a thoracic electrical bioimpedance (TEB) cardiac output monitor (Niccomo, Medis, Germany). A 3-min PLR was carried out before and after fluid infusion. Stroke volume changes (ΔSV) were calculated and a positive response was defined as ≥ 15% increase.
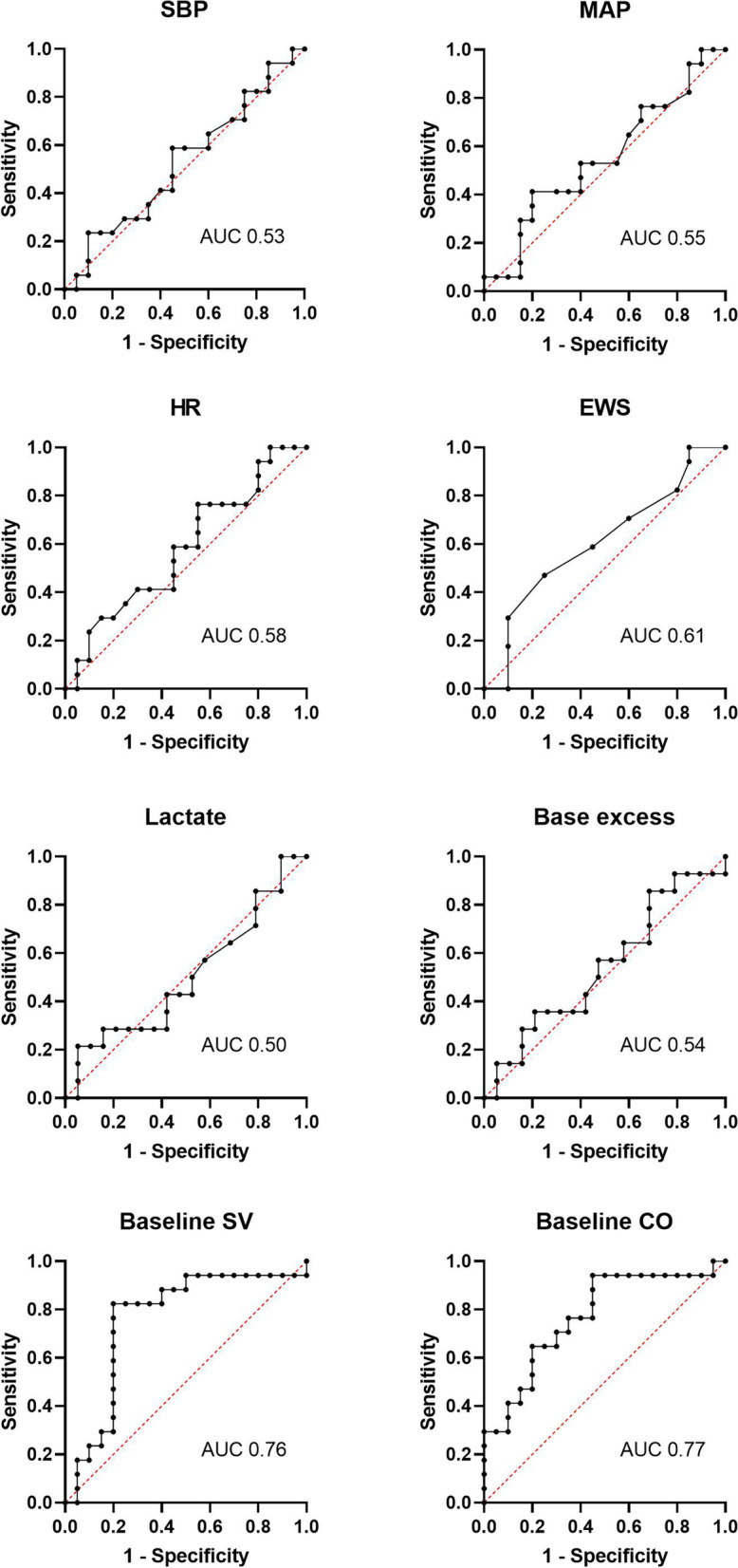
Results: We recruited 39 patients, of which 37 were included into the analysis. The median age was 63 (50-77) years and 19 patients were females. 17 patients (46%) were fluid responders compared to 11 (30%) with positive response to PLR1. ΔSV with PLR1 and fluid bolus showed moderate correlation (r = 0.47, 95% confidence interval, CI 0.17-0.69) and 62% concordance rate. For the prediction of the response to a fluid bolus the PLR test had a sensitivity of 41% (95% CI 22-64) and specificity of 80% (95% CI 58-92) with an area under the curve of 0.59 (95% CI 0.41-0.78). None of the standard parameters showed a better predictive ability compared to PLR.
Conclusion: Using TEB, ΔSV with PLR showed a moderate correlation with fluid bolus, with a limited accuracy to predict fluid responsiveness. The PLR test was a better predictor of fluid responsiveness than the parameters commonly used in emergency care (such as heart rate and blood pressure). These data suggest the potential for a clinical trial in sepsis comparing TEB monitored, PLR directed fluid management with standard care.
Keywords: Bioimpedance; Emergency; Fluid therapy; Haemodynamics; Non-invasive monitoring; Preload responsiveness.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Powell MF, Mathru M, Brandon A, et al. Assessment of endothelial glycocalyx disruption in term parturients receiving a fluid bolus before spinal anesthesia: a prospective observational study. Int J Obstet Anesth. 2014;23(4):330–334. doi: 10.1016/j.ijoa.2014.06.001[publishedOnlineFirst:2014/09/10]. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
