

Advances in Musculoskeletal Imaging in Juvenile Idiopathic Arthritis
- PMID: 36289680
- PMCID: PMC9598961
- DOI: 10.3390/biomedicines10102417
Advances in Musculoskeletal Imaging in Juvenile Idiopathic Arthritis
Abstract
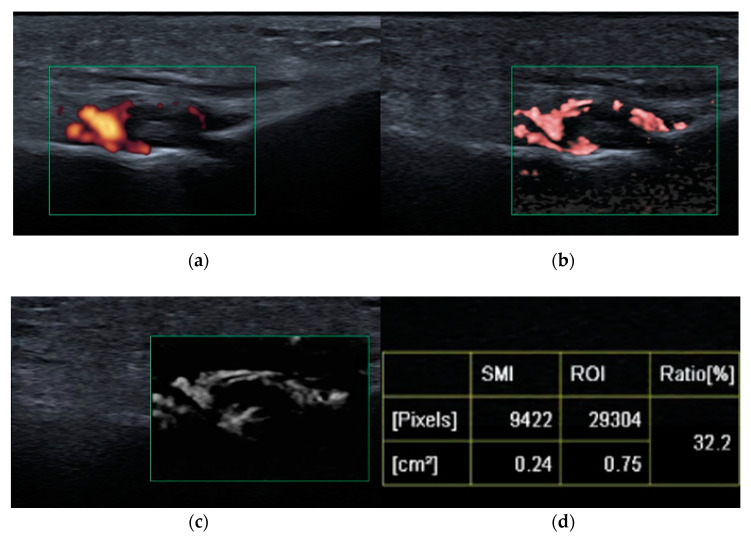
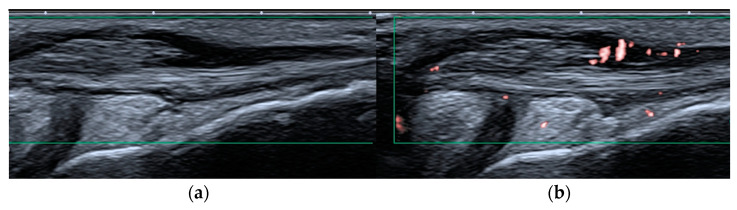
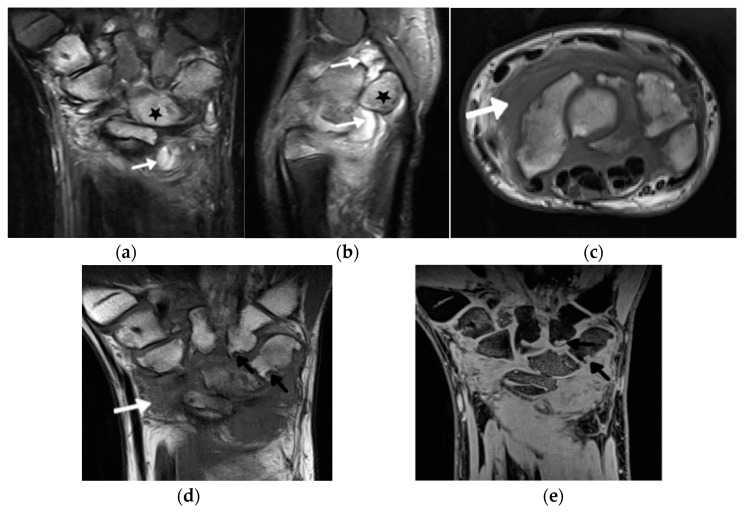
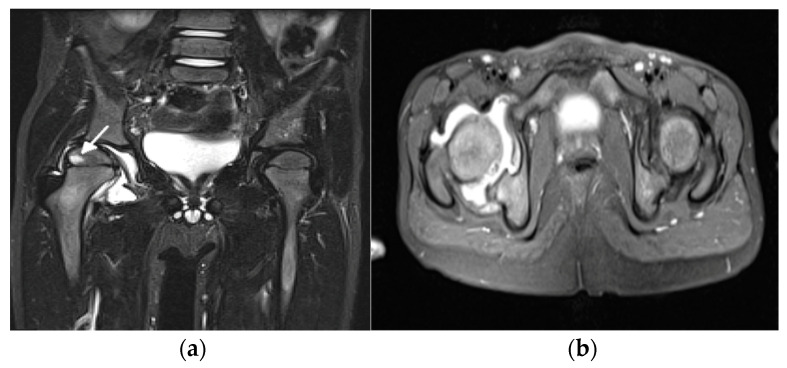
Over the past decade, imaging of inflammatory arthritis in juvenile arthropathies has significantly advanced due to technological improvements in the imaging modalities and elaboration of imaging recommendations and protocols through systematic international collaboration. This review presents the latest developments in ultrasound (US) and magnetic resonance imaging (MRI) of the peripheral and axial joints in juvenile idiopathic arthritis. In the field of US, the ultra-wideband and ultra-high-frequency transducers provide outstanding spatial resolution. The more sensitive Doppler options further improve the assessment and quantification of the vascularization of inflamed tissues, and shear wave elastography enables the diagnosis of tissue stiffness. Concerning MRI, substantial progress has been achieved due to technological improvements in combination with the development of semiquantitative scoring systems for the assessment of inflammation and the introduction of new definitions addressing the pediatric population. New solutions, such as superb microflow imaging, shear wave elastography, volume-interpolated breath-hold examination, and MRI-based synthetic computed tomography open new diagnostic possibilities and, at the same time, pose new challenges in terms of clinical applications and the interpretation of findings.
Keywords: elastography; juvenile idiopathic arthritis; magnetic resonance imaging; ultrasonography.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Lovell D.J. Juvenile idiopathic arthritis: Clinical features. In: Klippel J.H., Stone J.H., Crofford L.J., White P.F., editors. Primer on the Rheumatic Diseases. Springer; New York, NY, USA: 2008. pp. 142–148.
-
- El-Azeem M.I.A., Taha H.A., El-Sherif A.M. Role of MRI in evaluation of hip joint involvement in juvenile idiopathic arthritis. Egypt. Rheumatol. 2012;34:75–82. doi: 10.1016/j.ejr.2012.03.001. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
