

Exploring Antimicrobial Stewardship Influential Interventions on Improving Antibiotic Utilization in Outpatient and Inpatient Settings: A Systematic Review and Meta-Analysis
- PMID: 36289964
- PMCID: PMC9598859
- DOI: 10.3390/antibiotics11101306
Exploring Antimicrobial Stewardship Influential Interventions on Improving Antibiotic Utilization in Outpatient and Inpatient Settings: A Systematic Review and Meta-Analysis
Abstract
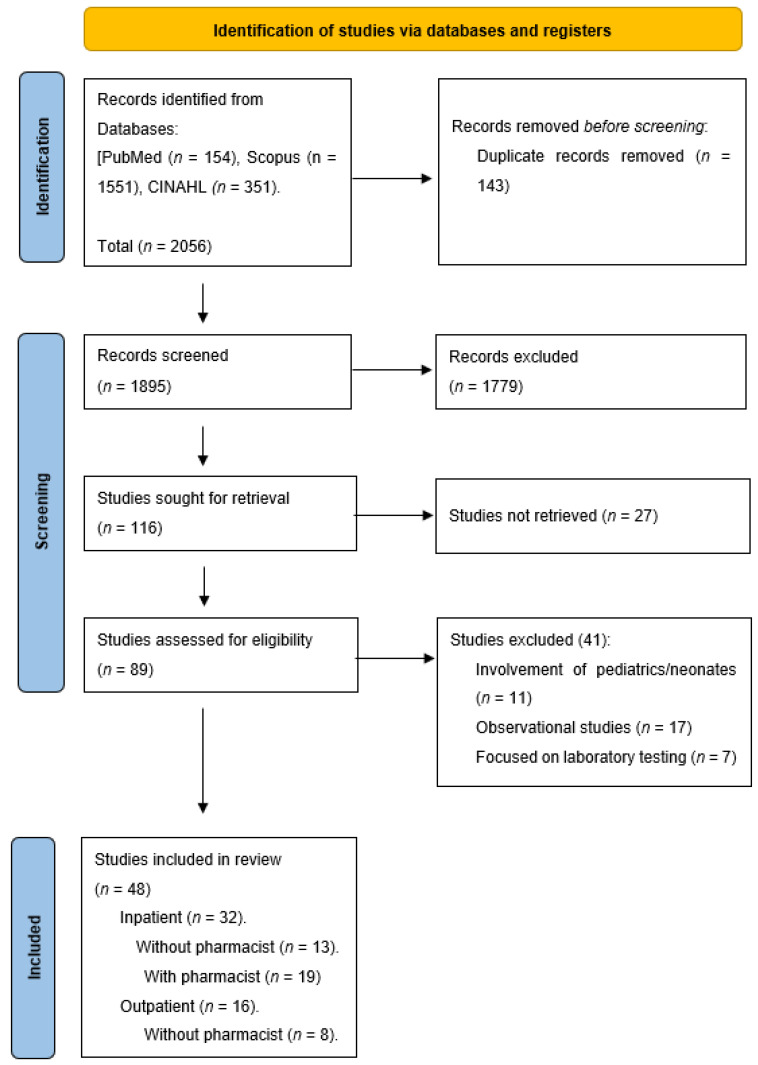
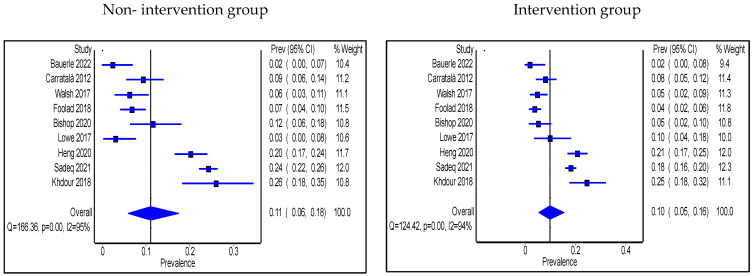
Antimicrobial stewardship interventions are targeted efforts by healthcare organizations to optimize antimicrobial use in clinical practice. The study aimed to explore effective interventions in improving antimicrobial use in hospitals. Literature was systemically searched for interventional studies through PubMed, CINAHL, and Scopus databases that were published in the period between January 2010 to April 2022. A random-effects model was used to pool and evaluate data from eligible studies that reported antimicrobial stewardship (AMS) interventions in outpatient and inpatient settings. Pooled estimates presented as proportions and standardized mean differences. Forty-eight articles were included in this review: 32 in inpatient and 16 in outpatient settings. Seventeen interventions have been identified, and eight outcomes have been targeted. AMS interventions improved clinical, microbiological, and cost outcomes in most studies. When comparing non-intervention with intervention groups using meta-analysis, there was an insignificant reduction in length of stay (MD: -0.99; 95% CI: -2.38, 0.39) and a significant reduction in antibiotics' days of therapy (MD: -2.73; 95% CI: -3.92, -1.54). There were noticeable reductions in readmissions, mortality rates, and antibiotic prescriptions post antimicrobial stewardship multi-disciplinary team (AMS-MDT) interventions. Studies that involved a pharmacist as part of the AMS-MDT showed more significant improvement in measured outcomes than the studies that did not involve a pharmacist.
Keywords: antimicrobial stewardship; antimicrobial use; clinical practice; interventions; multidisciplinary team.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- Micek S.T., Welch E.C., Khan J., Pervez M., Doherty J.A., Reichley R.M., Kollef M.H. Empiric combination antibiotic therapy is associated with improved outcome against sepsis due to Gram-negative bacteria: A retrospective analysis. Antimicrob. Agents Chemother. 2010;54:1742–1748. doi: 10.1128/AAC.01365-09. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
