

Long-Term Follow-Up, Treatment Strategies, Functional Outcome, and Health-Related Quality of Life after Surgery for WHO Grade 2 and 3 Intracranial Meningiomas
- PMID: 36291821
- PMCID: PMC9600120
- DOI: 10.3390/cancers14205038
Long-Term Follow-Up, Treatment Strategies, Functional Outcome, and Health-Related Quality of Life after Surgery for WHO Grade 2 and 3 Intracranial Meningiomas
Abstract
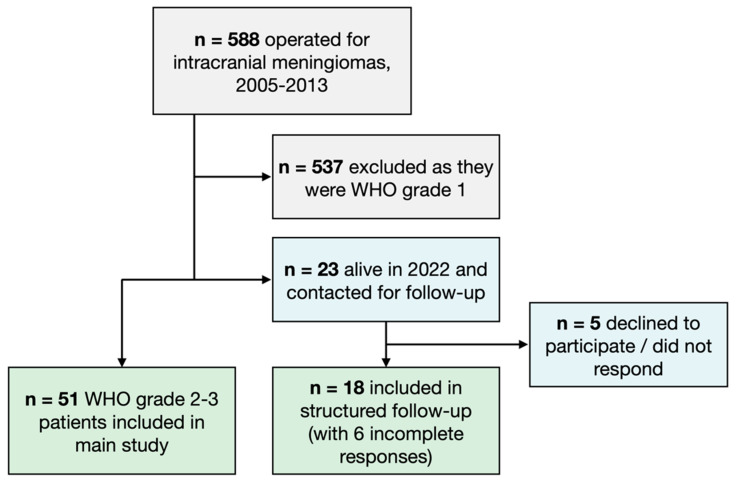
Progression-free survival (PFS) and overall survival (OS) for WHO grade 2 and 3 intracranial meningiomas are poorly described, and long-term results and data evaluating the routine use of supplementary fractionated radiotherapy (RT) or stereotactic radiosurgery (SRS) has been inconclusive. The aim of this study was to determine the long-term PFS and OS at a center that does not employ routine adjuvant RT. For this purpose, a retrospective population-based cohort study was conducted of all WHO grade 2 and 3 meningiomas surgically treated between 2005 and 2013. The cohort was uniformly defined according to the WHO 2007 criteria to allow comparisons to previously published reports. Patient records were reviewed, and patients were then prospectively contacted for structured quality-of-life assessments. In total, 51 consecutive patients were included, of whom 43 were WHO grade 2 and 8 were grade 3. A Simpson grade 1-2 resection was achieved in 62%. The median PFS was 31 months for grade 2 tumors, and 3.4 months for grade 3. The median OS was 13 years for grade 2, and 1.4 years for grade 3. The MIB-1-index was significantly associated with an increased risk for recurrence (p = 0.018, OR 1.12). The median PFS was significantly shorter for high-risk tumors compared to the low-risk group (10 vs. 46 months; p = 0.018). The surviving meningioma patients showed HRQoL measures comparable to that of the general population, with the exception of significantly more anxiety and depression. All patients who worked before surgery returned to work after their treatment. In conclusion, we confirm dismal prognoses in patients with grade 2 and 3 meningiomas, with tumor-related deaths resulting in severely reduced OS. However, the cohort was heterogenous, and a large subgroup of both grade 2 and 3 meningiomas was alive at 10 years follow-up, suggesting that a cure is possible. In addition, fractionated radiotherapy and chemotherapy had little benefit when introduced for recurrent and progressive diseases.
Keywords: WHO grade 2; WHO grade 3; chemotherapy; gamma-knife radiosurgery; health-related quality of life; meningioma; neurosurgery; patient-reported outcomes; radiotherapy; return to work.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Analysis of the results of recurrent intracranial meningiomas treated with re-radiosurgery.Clin Neurol Neurosurg. 2017 Feb;153:93-101. doi: 10.1016/j.clineuro.2016.12.014. Epub 2016 Dec 29. Clin Neurol Neurosurg. 2017. PMID: 28081463
-
Stereotactic radiosurgery versus stereotactic radiotherapy in the management of intracranial meningiomas: a systematic review and meta-analysis.Neurosurg Focus. 2019 Jun 1;46(6):E2. doi: 10.3171/2019.3.FOCUS1970. Neurosurg Focus. 2019. PMID: 31153149
-
Stereotactic radiosurgery in the treatment of parasellar meningiomas: long-term volumetric evaluation.J Neurosurg. 2018 Feb;128(2):362-372. doi: 10.3171/2016.11.JNS161402. Epub 2017 Mar 24. J Neurosurg. 2018. PMID: 28338439
-
Stereotactic radiosurgery of meningiomas following resection: predictors of progression.J Clin Neurosci. 2015 Jan;22(1):161-5. doi: 10.1016/j.jocn.2014.07.028. Epub 2014 Nov 7. J Clin Neurosci. 2015. PMID: 25439747
-
Meningiomas engaging major venous sinuses.World Neurosurg. 2014 Jan;81(1):116-24. doi: 10.1016/j.wneu.2013.01.095. Epub 2013 Jan 30. World Neurosurg. 2014. PMID: 23376533 Review.
Cited by
-
Long-term health-related quality of life in meningioma survivors: A mixed-methods systematic review.Neurooncol Adv. 2024 Jan 19;6(1):vdae007. doi: 10.1093/noajnl/vdae007. eCollection 2024 Jan-Dec. Neurooncol Adv. 2024. PMID: 38375359 Free PMC article.
-
Health-related quality-of-life outcomes in CNS WHO grade 2 and 3 meningioma: a systematic review.Neurosurg Rev. 2025 Feb 27;48(1):268. doi: 10.1007/s10143-025-03420-5. Neurosurg Rev. 2025. PMID: 40011234 Free PMC article.
-
Analysis of demographics and the impact of adjuvant radiotherapy on a nationwide cohort of patients with high-grade spinal meningiomas.Neurooncol Adv. 2024 Feb 5;6(1):vdae018. doi: 10.1093/noajnl/vdae018. eCollection 2024 Jan-Dec. Neurooncol Adv. 2024. PMID: 38410135 Free PMC article.
-
Giant Extracranial Meningioma Associated With Hormonal Imbalances Due to Thyroidectomy: Case Report and Literature Review.Cureus. 2023 Dec 31;15(12):e51376. doi: 10.7759/cureus.51376. eCollection 2023 Dec. Cureus. 2023. PMID: 38293000 Free PMC article.
-
Health-related quality of life in surgically treated asymptomatic meningioma patients: A population-based matched cohort study.Neurooncol Pract. 2024 Nov 15;11(6):723-732. doi: 10.1093/nop/npae047. eCollection 2024 Dec. Neurooncol Pract. 2024. PMID: 39554792 Free PMC article.
References
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
