

Perspectives in Therapy of Chronic Rhinosinusitis
- PMID: 36291990
- PMCID: PMC9600269
- DOI: 10.3390/diagnostics12102301
Perspectives in Therapy of Chronic Rhinosinusitis
Abstract
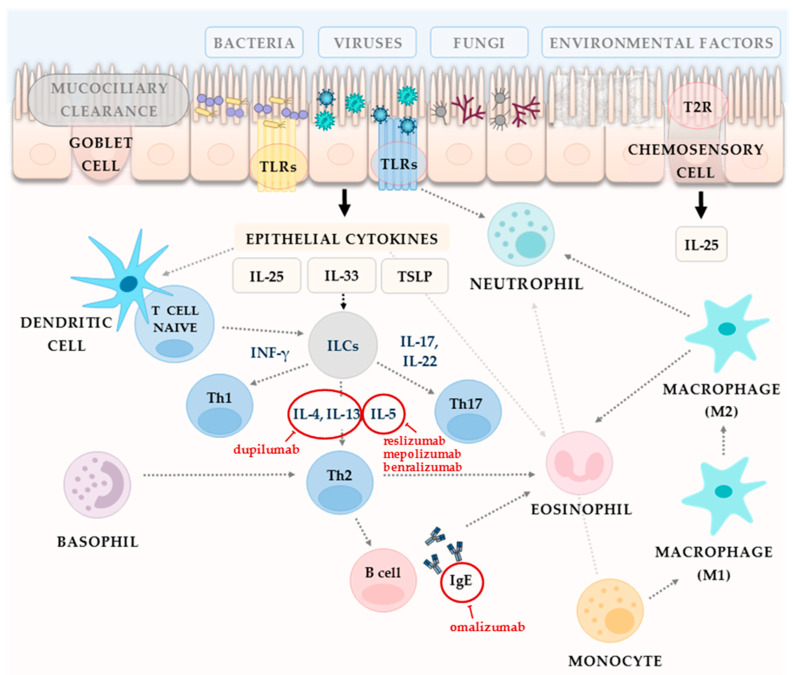
The recent classification of chronic rhinosinusitis (CRS) focusses on investigating underlying immunopathophysiological mechanisms. Primary CRS is subdivided based on endotype dominance into type 2 (that relates mostly to the Th2 immune response with high levels of IL-5, IL-13, and IgE), or non-type 2 (that corresponds to the mix of type 1 and type 3). The treatment selection of CRS is dependent on endotype dominance. Currently, the majority of patients receive standardized care-traditional pharmacological methods including local or systemic corticosteroids, nasal irrigations or antibiotics (for a selected group of patients). If well-conducted drug therapy fails, endoscopic sinus surgery is conducted. Aspirin treatment after aspirin desensitization (ATAD) with oral aspirin is an option for the treatment in nonsteroidal anti-inflammatory drug (NSAID)-exacerbated respiratory disease (N-ERD) patients. However, in this review the focus is on the role of biological treatment-monoclonal antibodies directed through the specific type 2 immune response targets. In addition, potential targets to immunotherapy in CRS are presented. Hopefully, effective diagnostic and therapeutic solutions, tailored to the individual patient, will be widely available very soon.
Keywords: biologics; chronic rhinosinusitis; sinusitis; treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Khan A., Vandeplas G., Huynh T., Joish V., Mannent L., Tomassen P., Van Zele T., Cardell L., Arebro J., Olze H., et al. The Global Allergy and Asthma European Network (GALEN rhinosinusitis cohort: A large European cross-sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinol. J. 2019;57:32–42. doi: 10.4193/Rhin17.255. - DOI - PubMed
-
- Marseglia G.L., Caimmi S., Marseglia A., Poddighe D., Leone M., Caimmi D., Ciprandi G., Castellazzi A.M. Rhinosinusitis and asthma. Int. J. Immunopathol. Pharmacol. 2010;23:29–31. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
