

The Prognostic Value of Ultrasound Findings in Preoperatively Distinguishing between Uncomplicated and Complicated Types of Pediatric Acute Appendicitis Based on Correlation with Intraoperative and Histopathological Findings
- PMID: 36292004
- PMCID: PMC9600393
- DOI: 10.3390/diagnostics12102315
The Prognostic Value of Ultrasound Findings in Preoperatively Distinguishing between Uncomplicated and Complicated Types of Pediatric Acute Appendicitis Based on Correlation with Intraoperative and Histopathological Findings
Abstract
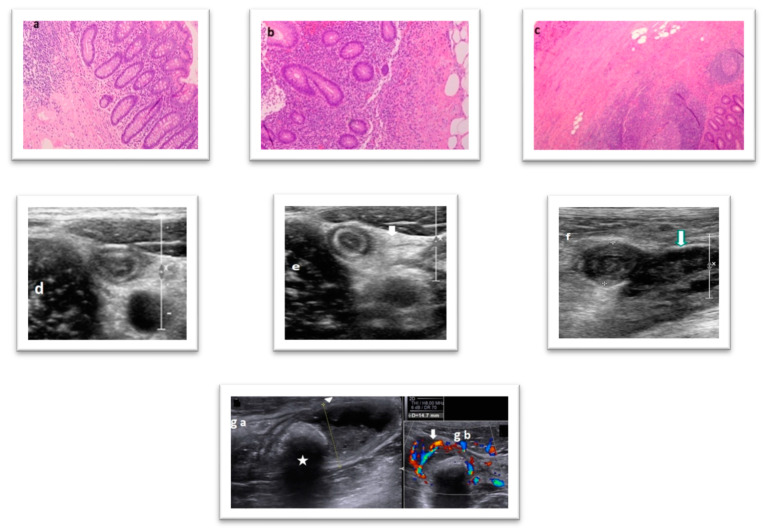
Objective: This study compares the preoperative ultrasound findings of all children with a clinical picture of acute appendicitis on the basis of intraoperative and histopathological findings to assess the feasibility of this approach in preoperatively distinguishing between uncomplicated and complicated cases.
Methods: This retrospective study includes 224 pediatric patients who underwent ultrasound prior to appendectomy at our institution between January 2016 and February 2022. Logistic regression analysis was used to investigate the association between sonographic and intraoperative histopathological findings.
Results: Of the 224 participants, 61.1% were intraoperatively diagnosed with uncomplicated appendicitis (59.8% male). Multivariate logistic regression analysis revealed that patients with a higher appendiceal diameter, presence of appendicolith, and peritonitis were more likely to suffer from complicated appendicitis. Finally, the common anatomical position of the appendix and an appendiceal diameter greater than 6 mm had the highest sensitivity (94.6% and 94.5%, respectively) for predicting complicated appendicitis, with the most specific (99.3%) sonographic finding being the existence of an abscess.
Conclusions: Preoperative abdominal ultrasound in children with a clinical diagnosis of acute appendicitis can distinguish between uncomplicated and complicated appendicitis in most cases of pediatric appendicitis. A higher appendiceal diameter, the presence of appendicolith, and peritonitis are parameters noted by ultrasound that strongly predict complicated appendicitis.
Keywords: complicated appendicitis; ultrasound; uncomplicated appendicitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Sonographic differentiation of complicated from uncomplicated appendicitis.Br J Radiol. 2019 Jul;92(1099):20190102. doi: 10.1259/bjr.20190102. Epub 2019 May 29. Br J Radiol. 2019. PMID: 31112397 Free PMC article.
-
Comparative study of imaging features in uncomplicated and complicated acute appendicitis.Ulus Travma Acil Cerrahi Derg. 2024 Oct;30(10):722-728. doi: 10.14744/tjtes.2024.50363. Ulus Travma Acil Cerrahi Derg. 2024. PMID: 39382365 Free PMC article.
-
Comparison of ultrasound assisted and intraoperative diameter measurement in acute appendicitis.Clin Anat. 2025 May;38(4):456-461. doi: 10.1002/ca.24227. Epub 2024 Sep 18. Clin Anat. 2025. PMID: 39295247
-
Histological analysis of appendices removed during interval appendectomy after conservative management of pediatric patients with acute appendicitis with an inflammatory mass or abscess.Surg Today. 2014 Aug;44(8):1400-5. doi: 10.1007/s00595-014-0950-0. Epub 2014 Jun 17. Surg Today. 2014. PMID: 24931545 Review.
-
Pathologic continuum of acute appendicitis: sonographic findings and clinical management implications.Ultrasound Q. 2011 Jun;27(2):71-9. doi: 10.1097/RUQ.0b013e31821b6eea. Ultrasound Q. 2011. PMID: 21606789 Review.
Cited by
-
Predicting severity of acute appendicitis with machine learning methods: a simple and promising approach for clinicians.BMC Emerg Med. 2024 Jun 18;24(1):101. doi: 10.1186/s12873-024-01023-9. BMC Emerg Med. 2024. PMID: 38886641 Free PMC article.
-
The application value of high-frequency ultrasound in the feasibility assessment of endoscopic retrograde appendicitis therapy in children with appendicitis.Sci Rep. 2023 Nov 7;13(1):19291. doi: 10.1038/s41598-023-46387-3. Sci Rep. 2023. PMID: 37935754 Free PMC article.
-
A Novel Deep Learning Approach for the Automatic Diagnosis of Acute Appendicitis.J Clin Med. 2024 Aug 22;13(16):4949. doi: 10.3390/jcm13164949. J Clin Med. 2024. PMID: 39201090 Free PMC article.
-
Predicting Complicated Appendicitis in Children: Pros and Cons of a New Score Combining Clinical Signs, Laboratory Values, and Ultrasound Images (CLU Score).Diagnostics (Basel). 2023 Jul 5;13(13):2275. doi: 10.3390/diagnostics13132275. Diagnostics (Basel). 2023. PMID: 37443669 Free PMC article.
-
Ultrasound and computed tomography in differentiating between simple and complicated appendicitis in pediatric patients.Pediatr Surg Int. 2024 Nov 9;40(1):299. doi: 10.1007/s00383-024-05880-0. Pediatr Surg Int. 2024. PMID: 39520568
References
-
- James C.Y. Dunn. Appendicitis. In: Grosfeld J.L., O’Neill J.A. Jr., Coran A.G., Fonkalsrud E.W., Caldamone A.A., editors. Pediatric Surgery. 6th ed. Volume 2. Mosby Elsevier; Philadelphia, PA, USA: 2006. pp. 1501–1502.
-
- Gadiparthi R., Waseem M. StatPearls [Internet] StatPearls Publishing; Treasure Island, FL, USA: 2022. Pediatric Appendicitis. 2022 May 3. - PubMed
-
- Al-Khusheh M., Iqbal S., Gupta A.K., Asalieh H., Khalifa K., Habeeb K. The role of abdominal X-rays in the investigation of suspected acute appendicitis. J. Med. Med. Sci. 2011;2:1216–1220.
LinkOut - more resources
Full Text Sources
