

Autoimmune Pancreatitis: From Pathogenesis to Treatment
- PMID: 36293522
- PMCID: PMC9604056
- DOI: 10.3390/ijms232012667
Autoimmune Pancreatitis: From Pathogenesis to Treatment
Abstract
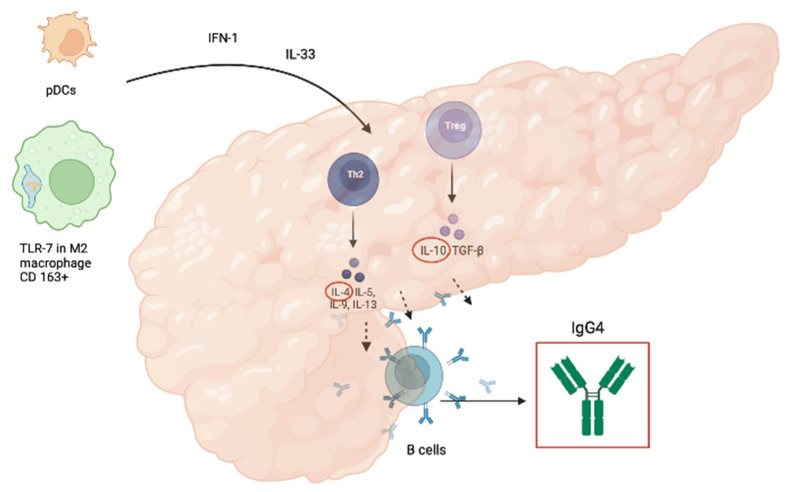
Autoimmune pancreatitis (AIP) is a rare disease. The diagnosis of AIP is difficult and should be made by a comprehensive evaluation of clinical, radiological, serological, and pathological findings. Two different types of AIP have been identified: autoimmune pancreatitis type 1 (AIP-1), which is considered a pancreatic manifestation of multiorgan disease related to IgG4, and autoimmune pancreatitis type 2 (AIP-2), which is considered a pancreas-specific disease not related to IgG4. Although the pathophysiological conditions seem to differ between type 1 and type 2 pancreatitis, both respond well to steroid medications. In this review, we focused on the pathogenesis of the disease to develop a tool that could facilitate diagnosis and lead to the discovery of new therapeutic strategies to combat autoimmune pancreatitis and its relapses. The standard therapy for AIP is oral administration of corticosteroids. Rituximab (RTX) has also been proposed for induction of remission and maintenance therapy in relapsing AIP-1. In selected patients, immunomodulators such as azathioprine are used to maintain remission. The strength of this review, compared with previous studies, is that it focuses on the clear difference between the two types of autoimmune pancreatitis with a clearly delineated and separate pathogenesis. In addition, the review also considers various therapeutic options, including biologic drugs, such as anti-tumor necrosis factor (TNF) therapy, a well-tolerated and effective second-line therapy for AIP type 2 relapses or steroid dependence. Other biologic therapies are also being explored that could provide a useful therapeutic alternative to corticosteroids and immunosuppressants, which are poorly tolerated due to significant side effects.
Keywords: AIP-1; AIP-2; IgG4-related disease; autoimmune pancreatitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Shimosegawa T., Chari S.T., Frulloni L., Kamisawa T., Kawa S., Mino-Kenudson M., Kim M.H., Klöppel G., Lerch M.M., Löhr M., et al. International Consensus Diagnostic Criteria for Autoimmune Pancreatitis: Guidelines of the International Association of Pancreatology. Pancreas. 2011;40:352–358. doi: 10.1097/MPA.0b013e3182142fd2. - DOI - PubMed
-
- Sah R.P., Chari S.T., Pannala R., Sugumar A., Clain J.E., Levy M.J., Pearson R.K., Smyrk T.C., Petersen B.T., Topazian M.D., et al. Differences in Clinical Profile and Relapse Rate of Type 1 Versus Type 2 Autoimmune Pancreatitis. Gastroenterology. 2010;139:140–148. doi: 10.1053/j.gastro.2010.03.054. - DOI - PubMed
-
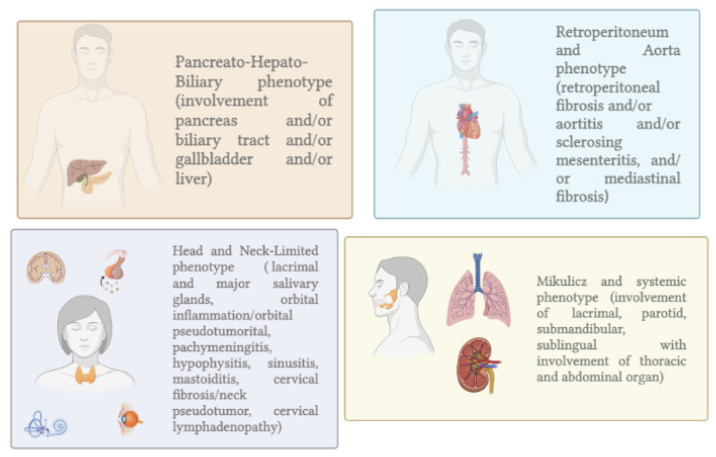
- Wallace Z.S., Zhang Y., Perugino C.A., Naden R., Choi H.K., Stone J.H., Takashi Akamizu C., Akiyama M., Bateman A., Blockmans D., et al. Clinical Phenotypes of IgG4-Related Disease: An Analysis of Two International Cross-Sectional Cohorts HHS Public Access. Eur. Leag. Against Rheum. 2018;77:70. doi: 10.1136/annrheumdis-2018-214603. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
