

The Transcriptomic Landscape of Pediatric Astrocytoma
- PMID: 36293551
- PMCID: PMC9604090
- DOI: 10.3390/ijms232012696
The Transcriptomic Landscape of Pediatric Astrocytoma
Abstract
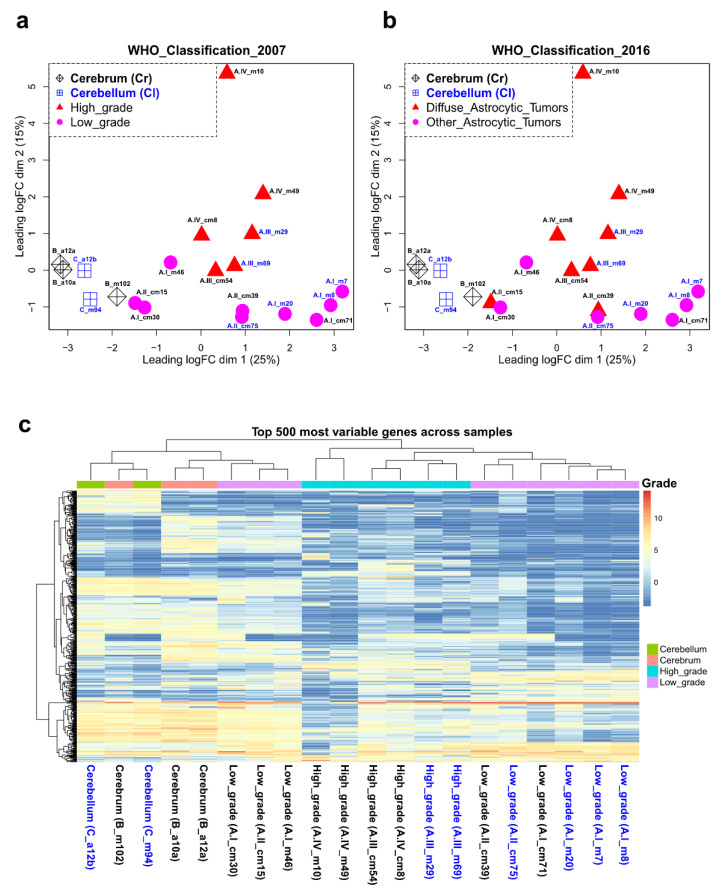
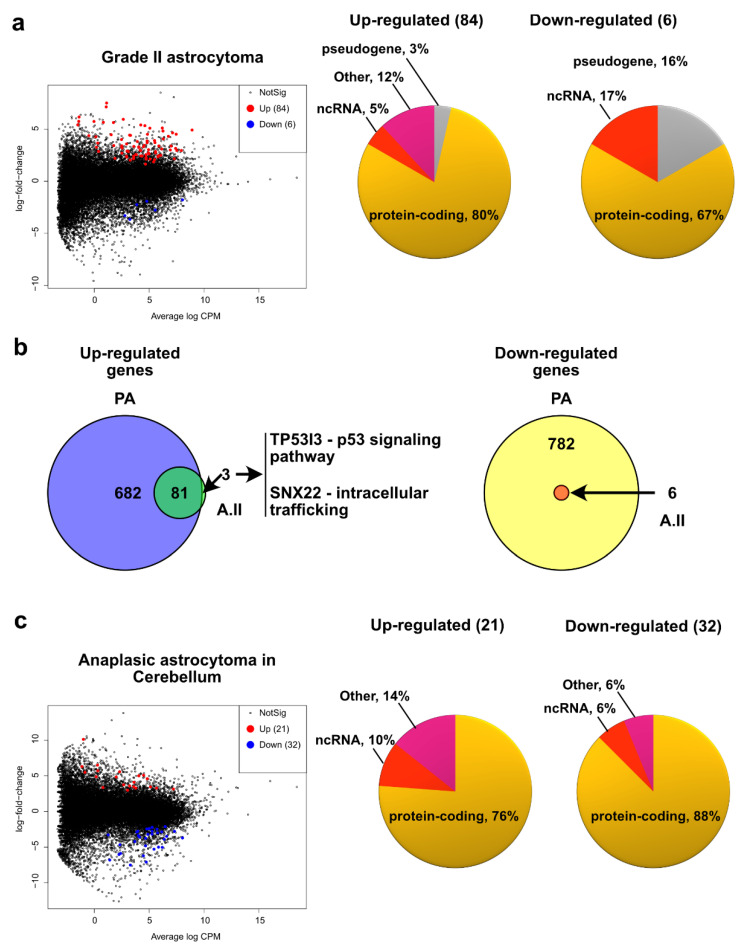
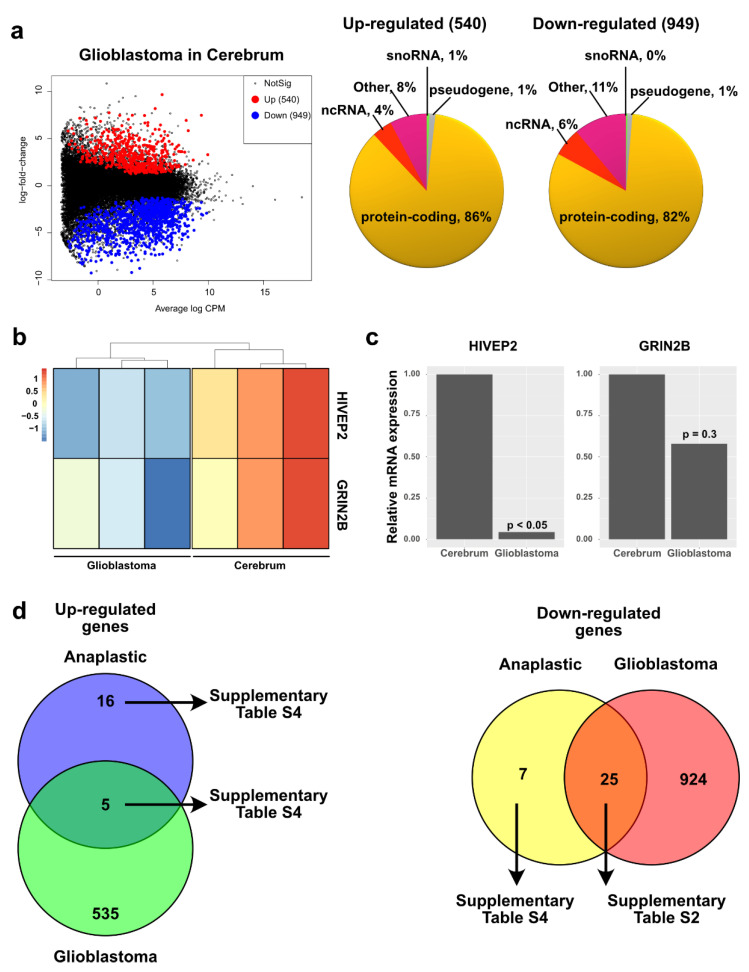
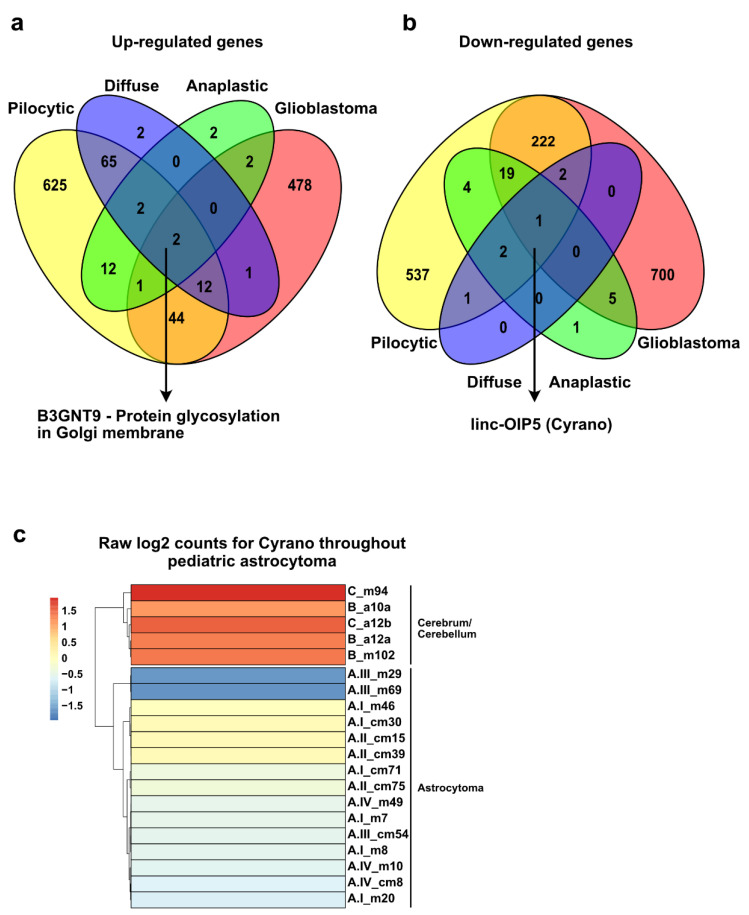
Central nervous system tumors are the most common solid neoplasia during childhood and represent one of the leading causes of cancer-related mortality. Tumors arising from astrocytic cells (astrocytomas) are the most frequently diagnosed, and according to their histological and pathological characteristics, they are classified into four categories. However, an additional layer of molecular classification considering the DNA sequence of the tumorigenesis-associated genes IDH1/2 and H3F3A has recently been incorporated into the classification guidelines. Although mutations in H3F3A are found exclusively in a subtype of grade IV pediatric astrocytoma, mutations in IDH1/2 genes are very rare in children under 14 years of age. The transcriptomic profiles of astrocytoma in adults and children have been extensively studied. However, there is scarce information on these profiles in pediatric populations considering the status of tumorigenesis-associated genes. Therefore, here we report the transcriptomic landscape of the four grades of pediatric astrocytoma by RNA sequencing. We found several well-documented biological functions associated with the misregulated genes in the four grades of astrocytoma, as well as additional biological pathways. Among the four grades of astrocytoma, we found shared misregulated genes that could have implications in tumorigenesis. Finally, we identified a transcriptional signature for almost all grades of astrocytoma that could be used as a transcription-based identification method.
Keywords: RNA-seq; pediatric astrocytoma; transcriptome.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Chico-Ponce de Leon F., Castro-Sierra E., Perezpena-Diazconti M., Gordillo-Dominguez L.F., Santana-Montero B.L., Rocha-Rivero L.E., Vaca-Ruiz M.E., Ríos-Alanís M., Sánchez-Herrera F., Valdés-Ordoño R. Pediatric Intracranial Tumors. Bol. Med. Hosp. Infant. Mex. 2016;63:367–381.
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
-
- PDQ Pediatric Treatment Editorial Board . PDQ Cancer Information Summaries. National Cancer Institute (US); Bethesda, MD, USA: 2002. Childhood Astrocytomas Treatment (PDQ(R)): Health Professional Version. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
