

Association of Health Status Metrics with Clinical Outcomes in Patients with Adult Congenital Heart Disease and Atrial Arrhythmias
- PMID: 36294501
- PMCID: PMC9605619
- DOI: 10.3390/jcm11206181
Association of Health Status Metrics with Clinical Outcomes in Patients with Adult Congenital Heart Disease and Atrial Arrhythmias
Abstract
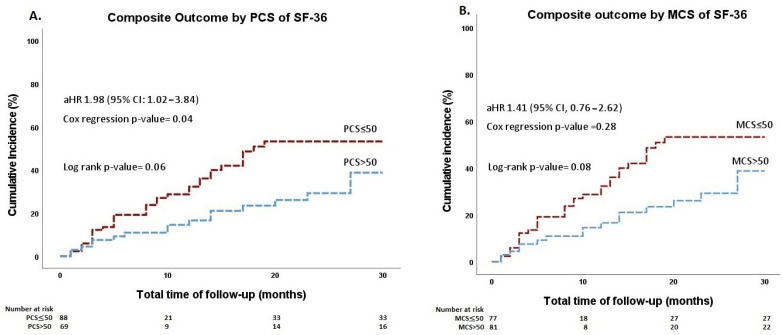
The prognostic value of health status metrics in patients with adult congenital heart disease (ACHD) and atrial arrhythmias is unclear. In this retrospective cohort study of an ongoing national, multicenter registry (PROTECT-AR, NCT03854149), ACHD patients with atrial arrhythmias on apixaban are included. At baseline, health metrics were assessed using the physical component summary (PCS), the mental component summary (MCS) of the Short-Form-36 (SF-36) Health Survey, and the modified European Heart Rhythm Association (mEHRA) score. Patients were divided into groups according to their SF-36 PCS and MCS scores, using the normalized population mean of 50 on the PCS and MCS as a threshold. The primary outcome was the composite of mortality from any cause, major thromboembolic events, major/clinically relevant non-major bleedings, or hospitalizations. Multivariable Cox-regression analyses using clinically relevant parameters (age greater than 60 years, anatomic complexity, ejection fraction of the systemic ventricle, and CHA₂DS₂-VASc and HAS-BLED scores) were performed to examine the association of health metrics with the composite outcome. Over a median follow-up period of 20 months, the composite outcome occurred in 50 of 158 (32%) patients. The risk of the outcome was significantly higher in patients with SF-36 PCS ≤ 50 compared with those with PCS > 50 (adjusted hazard ratio (aHR), 1.98; 95% confidence interval [CI], 1.02−3.84; p = 0.04) after adjusting for possible confounders. The SF-36 MCS ≤ 50 was not associated with the outcome. The mEHRA score was incrementally associated with a higher risk of the composite outcome (aHR = 1.44 per 1 unit increase in score; 95% CI, 1.03−2.00; p = 0.03) in multivariable analysis. In ACHD patients with atrial arrhythmias, the SF-36 PCS ≤ 50 and mEHRA scores predicted an increased risk of adverse events.
Keywords: ACHD; SF-36; atrial arrhythmia; congenital heart disease; mEHRA; quality of life.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the study design, collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication.
Figures
References
-
- Kempny A., Dimopoulos K., Uebing A., Moceri P., Swan L., Gatzoulis M.A., Diller G.P. Reference values for exercise limitations among adults with congenital heart disease. Relation to activities of daily lifesingle centre experience and review of published data. Eur. Heart J. 2012;33:1386–1396. doi: 10.1093/eurheartj/ehr461. - DOI - PubMed
-
- Koyak Z., Achterbergh R.C.A., De Groot J.R., Berger F., Koolbergen D.R., Bouma B.J., Lagrand W.K., Hazekamp M.G., Blom N.A., Mulder B.J.M. Postoperative arrhythmias in adults with congenital heart disease: Incidence and risk factors. Int. J. Cardiol. 2013;169:139–144. doi: 10.1016/j.ijcard.2013.08.087. - DOI - PubMed
-
- Hernández-Madrid A., Paul T., Abrams D., Aziz P.F., Blom N.A., Chen J., Chessa M., Combes N., Dagres N., Diller G., et al. Arrhythmias in congenital heart disease: A position paper of the European Heart Rhythm Association (EHRA), Association for European Paediatric and Congenital Cardiology (AEPC), and the European Society of Cardiology (ESC) Working Group on Grown-up Congeni. Europace. 2018;20:1719–1720. doi: 10.1093/europace/eux380. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
