

Hospitalisation Is Prognostic of Survival in Chronic Thromboembolic Pulmonary Hypertension
- PMID: 36294508
- PMCID: PMC9605547
- DOI: 10.3390/jcm11206189
Hospitalisation Is Prognostic of Survival in Chronic Thromboembolic Pulmonary Hypertension
Erratum in
-
Correction: Jansa et al. Hospitalisation Is Prognostic of Survival in Chronic Thromboembolic Pulmonary Hypertension. J. Clin. Med. 2022, 11, 6189.J Clin Med. 2023 Jun 9;12(12):3939. doi: 10.3390/jcm12123939. J Clin Med. 2023. PMID: 37373865 Free PMC article.
Abstract
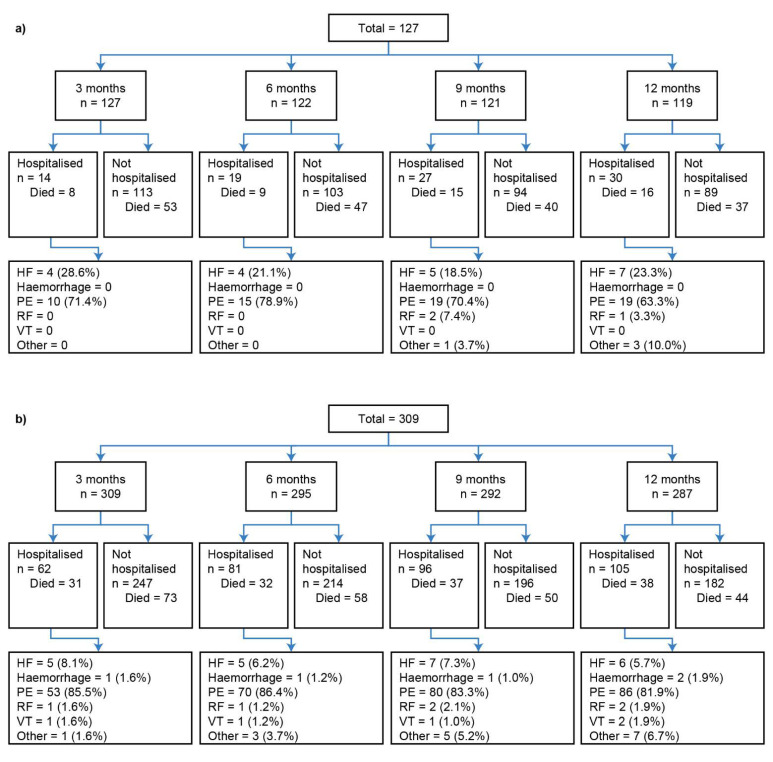
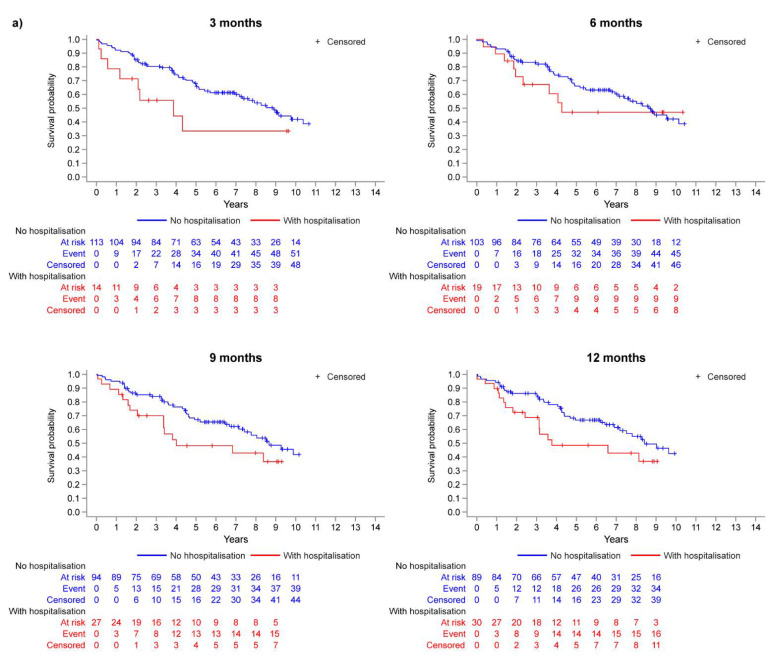
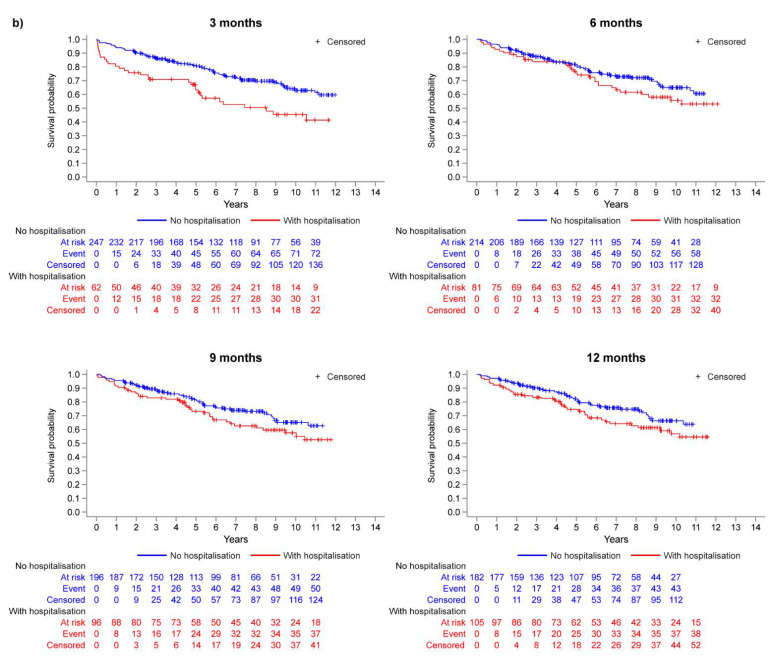
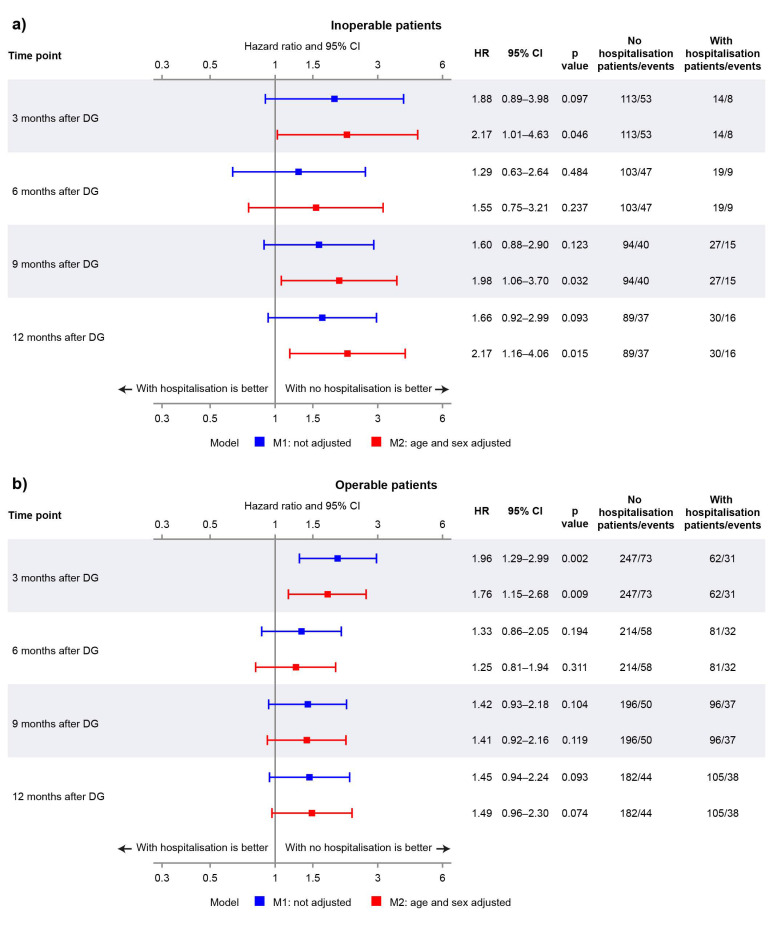
This analysis investigated the prognostic value of hospitalisation in chronic thromboembolic pulmonary hypertension (CTEPH) using data from the Czech Republic, wherein pulmonary endarterectomy (PEA) was the only targeted treatment option until 2015. Using a landmark method, this analysis quantified the association between a first CTEPH-related hospitalisation event occurring before 3-, 6-, 9-, and 12-month landmark timepoints and subsequent all-cause mortality in adult CTEPH patients diagnosed between 2003 and 2016 in the Czech Republic. Patients were stratified into operable and inoperable, according to PEA eligibility. CTEPH-related hospitalisations were defined as non-elective. Hospitalisations related to CTEPH diagnosis, PEA, balloon pulmonary angioplasty, or clinical trial participation were excluded. Of 436 patients who survived to ≥3 months post diagnosis, 309 were operable, and 127 were inoperable. Sex- and age-adjusted hazard ratios (HRs) showed CTEPH-related hospitalisation was a statistically significant prognostic indicator of mortality at 3, 9, and 12 months in inoperable patients, with an approximately 2-fold increased risk of death in the hospitalisation group (HRs [95% CI] ranging from 1.98 [1.06-3.70] to 2.17 [1.01-4.63]). There was also a trend of worse survival probabilities in the hospitalisation groups for operable patients, with the difference most pronounced at 3 months, with a 76% increased risk of death (adjusted HR [95% CI] 1.76 [1.15-2.68]). This first analysis on the prognostic value of CTEPH-related hospitalisations demonstrates that a first CTEPH-related hospitalisation is prognostic of mortality in CTEPH, particularly for inoperable patients. These patients may benefit from medical and/or interventional therapy.
Keywords: CTEPH-related morbidity; hospitalisation; mortality; prognosis; pulmonary endarterectomy; pulmonary hypertension.
Conflict of interest statement
Pavel Jansa has received fees and grants from Janssen Pharmaceutical Companies of Johnson and Johnson, AOP Orphan, Bayer Healthcare Pharmaceuticals, and MSD. Susan Edwards, Virginie Gressin, and Lilla Di Scala are employees of and have shares in Janssen, a pharmaceutical company of Johnson and Johnson. The remaining authors declare no conflicts of interest. Authors Susan Edwards, Virginie Gressin, and Lilla Di Scala (employees of study funders) had a role in the design of the study, analyses and interpretation of the data, in the writing and reviewing of the manuscript, and in the decision to publish the results.
Figures
References
-
- Galiè N., Humbert M., Vachiery J.L., Gibbs S., Lang I., Torbicki A., Simonneau G., Peacock A., Vonk Noordegraaf A., Beghetti M., et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Respir. J. 2015;46:903–975. doi: 10.1183/13993003.01032-2015. - DOI - PubMed
-
- Leber L., Beaudet A., Muller A. Epidemiology of pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: Identification of the most accurate estimates from a systematic literature review. Pulm Circ. 2021;11:2045894020977300. doi: 10.1177/2045894020977300. - DOI - PMC - PubMed
-
- Delcroix M., Lang I., Pepke-Zaba J., Jansa P., D’Armini A.M., Snijder R., Bresser P., Torbicki A., Mellemkjaer S., Lewczuk J., et al. Long-term outcome of patients with chronic thromboembolic pulmonary hypertension: Results from an international prospective registry. Circulation. 2016;133:859–871. doi: 10.1161/CIRCULATIONAHA.115.016522. - DOI - PubMed
-
- Quadery S.R., Swift A.J., Billings C.G., Thompson A.A., Elliot C.A., Hurdman J., Charalampopoulos A., Sabroe I., Armstrong I.J., Hamilton N., et al. The impact of patient choice on survival in chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2018;52:1800589. doi: 10.1183/13993003.00589-2018. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
