

Histomorphometrical and CBCT Evaluation of Tissue Loss Progression Induced by Consecutive, Alternate Ligatures in Experimental Peri-Implantitis in a Dog Model: A Pilot Study
- PMID: 36294510
- PMCID: PMC9605274
- DOI: 10.3390/jcm11206188
Histomorphometrical and CBCT Evaluation of Tissue Loss Progression Induced by Consecutive, Alternate Ligatures in Experimental Peri-Implantitis in a Dog Model: A Pilot Study
Abstract
Objectives: Soft and hard tissue breakdown was histologically and radiologically assessed around implants with alternate, consecutively placed ligatures on the same edentulous dog hemimandible. The influence of ligatured implants (LI) on adjacent non-ligatured implants (NLI, as a possible naturally induced peri-implantitis) was also evaluated.
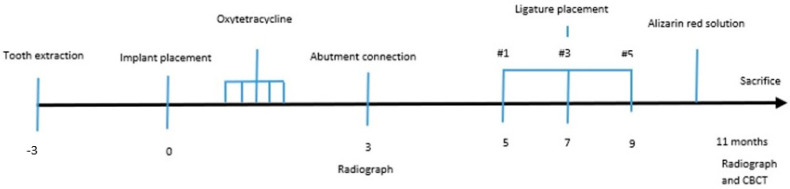
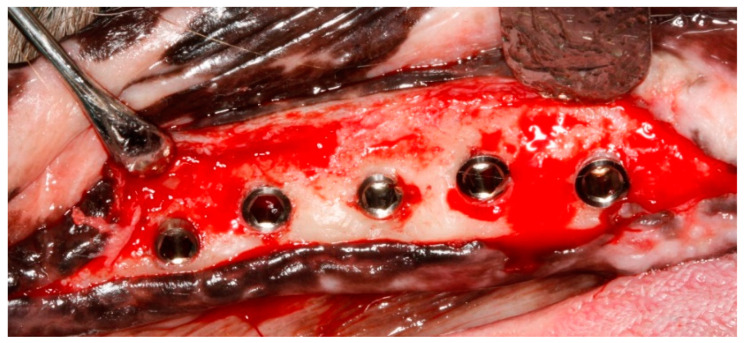
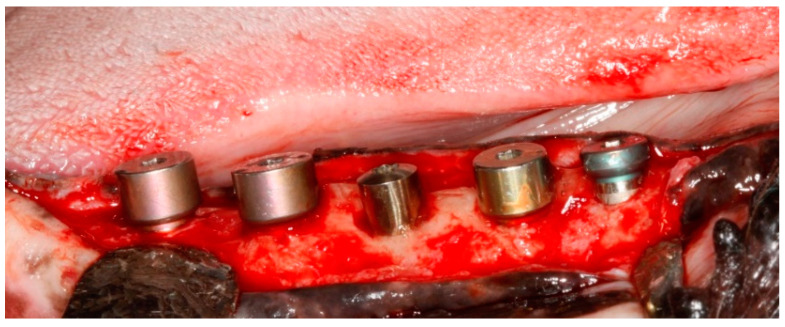
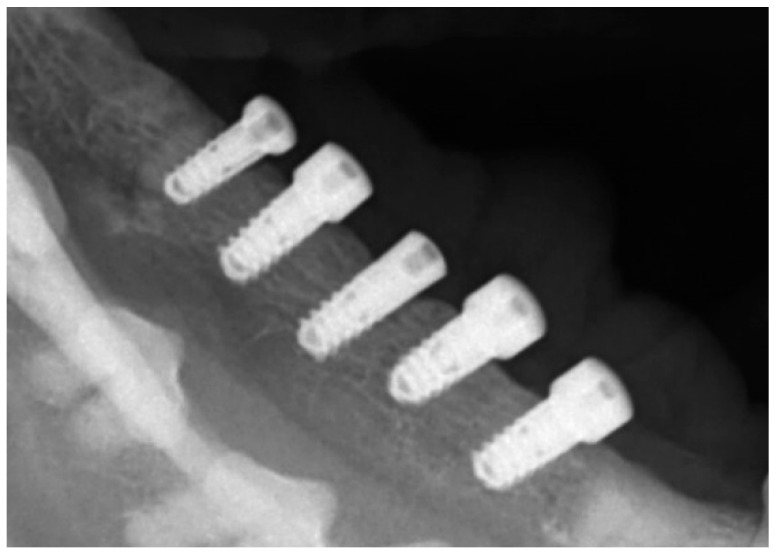
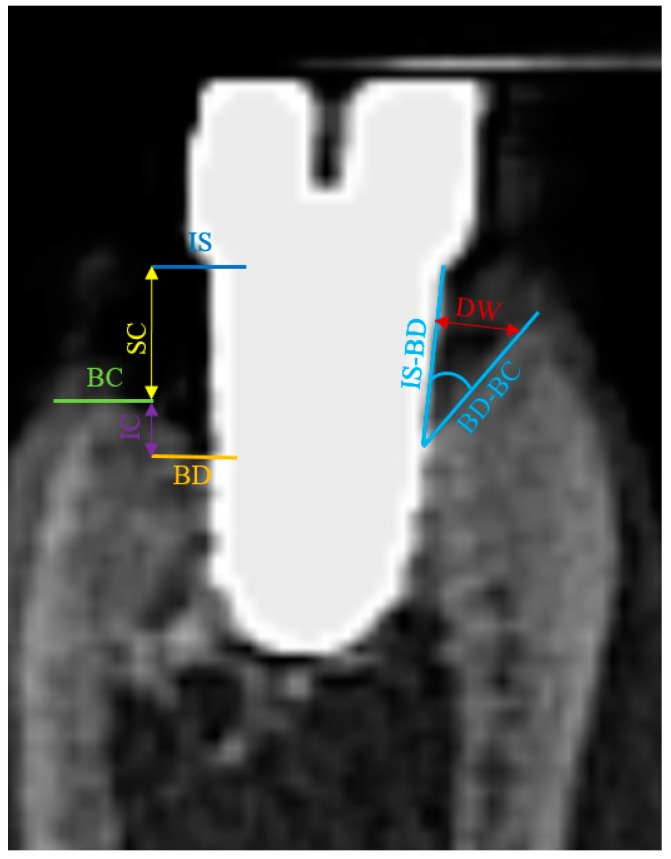
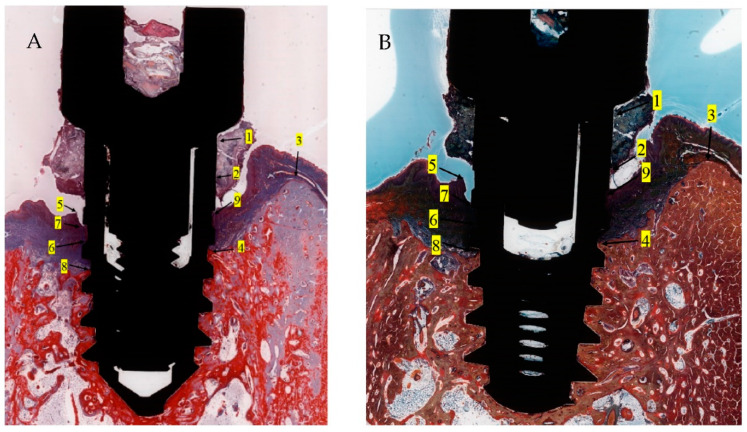
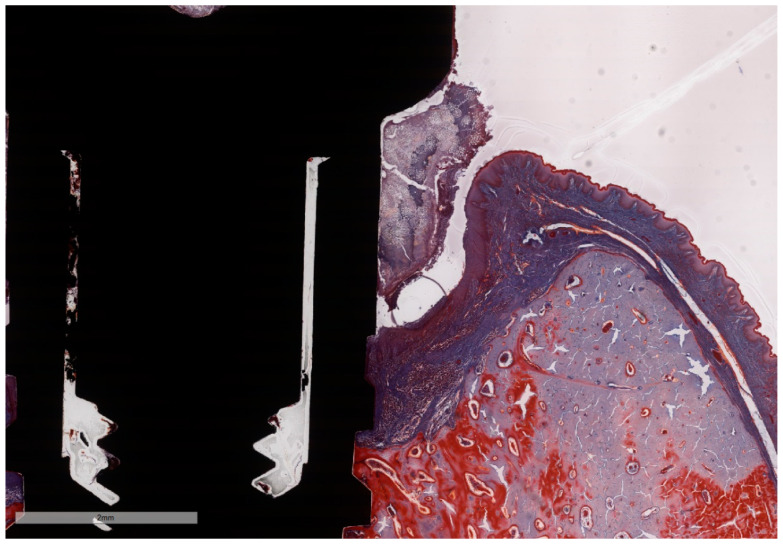
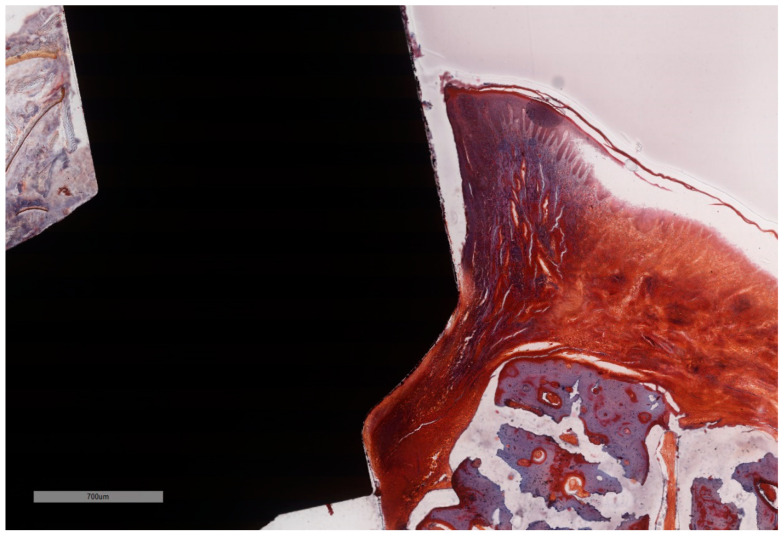
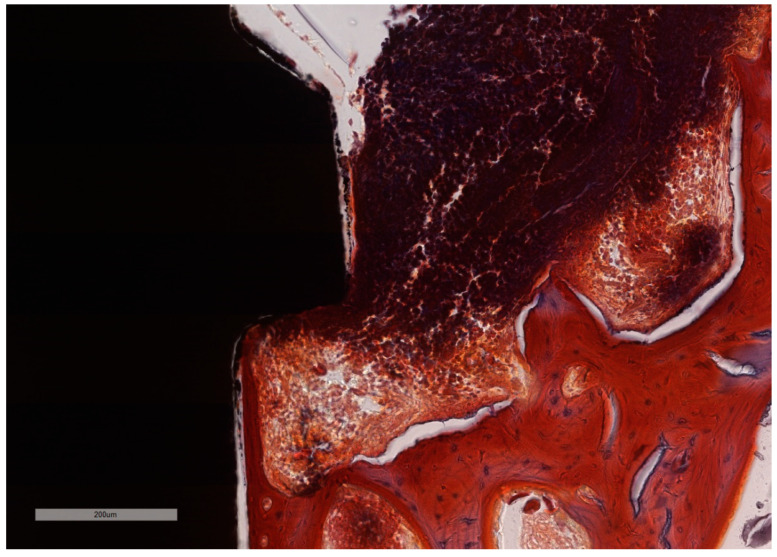
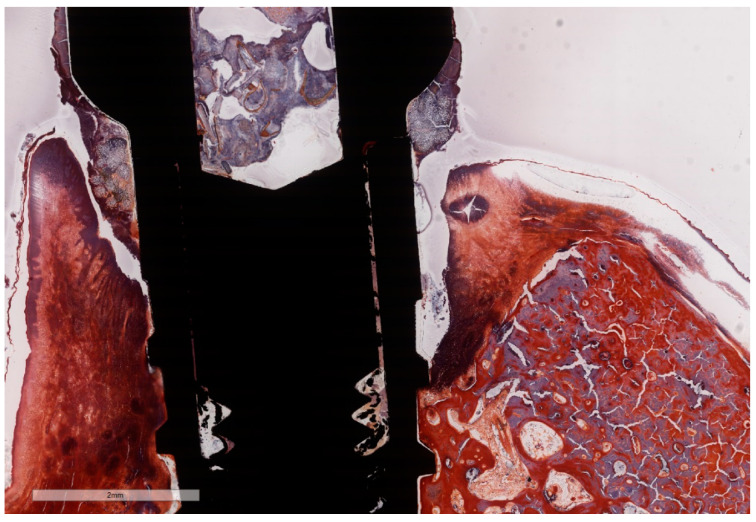
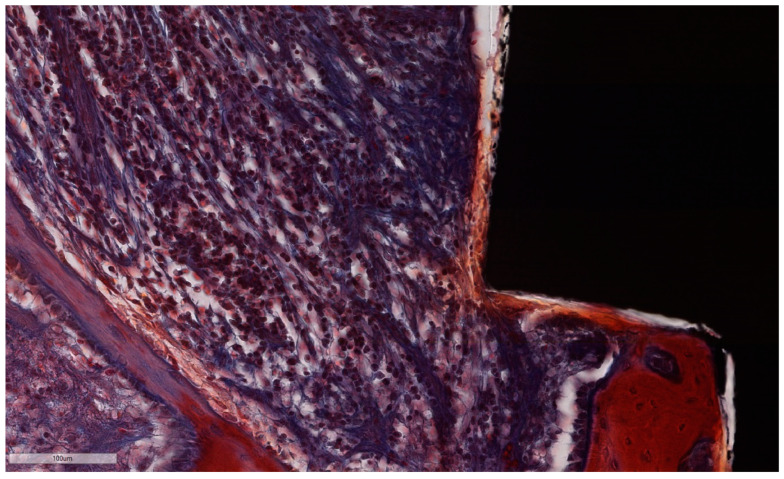
Material and methods: Three months after tooth extraction, five dental implants were placed in the dog hemimandible. Two months after abutment placement, ligatures were placed subsequently two months apart on alternate implants, while both intermediate implants were left without ligatures. Ligatures were kept in place during the entire experiment, and no plaque control measures were taken. Eleven months post-implantation, the animal was sacrificed. Undecalcified ground sections were cut, stained with Masson Goldner and MOVAT Pentachrome and evaluated by light microscopy. Soft and hard tissue loss was assessed using histomorphometric and CBCT parameters.
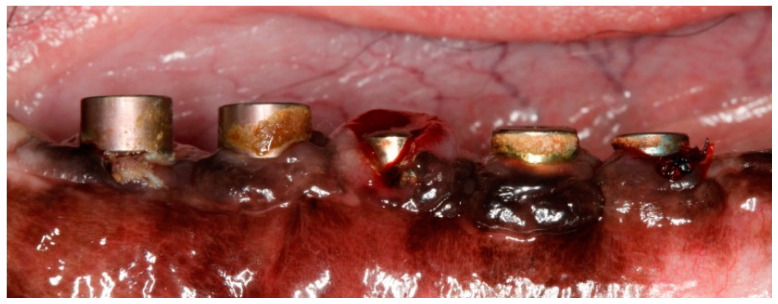
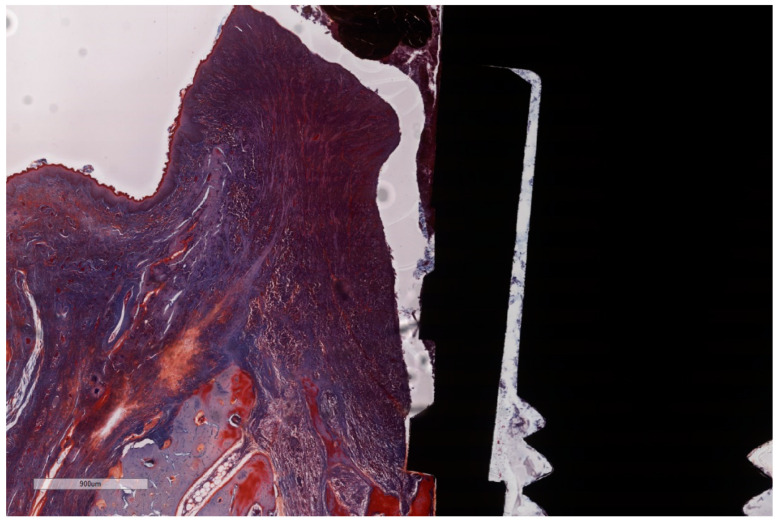
Results: All NLI presented deep false peri-implant pockets on the oral aspect and pronounced vertical bone resorption on the buccal aspect. After 2, 4 and 6 months, during the breakdown period, more than 30% of the bone was lost in LI in all directions, while, despite immediate vicinity, NLI displayed less destruction. Intense inflammation, typical for induced peri-implantitis, was present, with similar intensity in LI as NLI, but in different parts of the lesions. Morphometry confirmed intense soft tissue inflammation, more bone resorption and higher amounts of infiltrated connective tissue in LI when compared with NLI.
Conclusion: Within the limits of the present pilot study, the adequacy of the experimental dog model based on ligature-induced peri-implantitis was able to be successfully challenged by non-ligature models of spontaneously occurring peri-implant inflammation, while meeting the requirements for experimental designs with a very small numbers of animals. The influence of implants with severe peri-implantitis on adjacent implants resulted in less than expected tissue loss in the latter accession numbers.
Keywords: animal study; cone-beam CT; dental implant; histomorphometry; ligature induced; naturally occurring; peri-implantitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Influence of Section Thickness on the Accuracy and Specificity of Histometric Parameters Using Confocal Laser Scanning Microscopy in a Canine Model of Experimental Peri-Implantitis-A Proof of Concept.J Clin Med. 2023 Mar 23;12(7):2462. doi: 10.3390/jcm12072462. J Clin Med. 2023. PMID: 37048546 Free PMC article.
-
Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: an experimental study in dogs.Clin Oral Implants Res. 2007 Oct;18(5):655-61. doi: 10.1111/j.1600-0501.2007.01397.x. Epub 2007 Jun 30. Clin Oral Implants Res. 2007. PMID: 17608738
-
Hard tissue volumetric and soft tissue contour linear changes at implants with different surface characteristics after experimentally induced peri-implantitis: an experimental in vivo investigation.Clin Oral Investig. 2021 Jun;25(6):3905-3918. doi: 10.1007/s00784-020-03720-8. Epub 2021 Jan 7. Clin Oral Investig. 2021. PMID: 33415377
-
Are marginal bone level changes around dental implants due to infection?Clin Implant Dent Relat Res. 2021 Apr;23(2):170-177. doi: 10.1111/cid.12971. Epub 2021 Jan 18. Clin Implant Dent Relat Res. 2021. PMID: 33463079 Review.
-
Experimentally induced peri-implantitis: a review of different treatment methods described in the literature.Int J Oral Maxillofac Implants. 2000 Jul-Aug;15(4):533-44. Int J Oral Maxillofac Implants. 2000. PMID: 10960987 Review.
Cited by
-
Peri-implantitis with a potential axis to brain inflammation: an inferential review.Odontology. 2024 Oct;112(4):1033-1046. doi: 10.1007/s10266-024-00936-y. Epub 2024 Apr 17. Odontology. 2024. PMID: 38630323 Review.
-
Peri-Implant Microbial Signature Shifts in Titanium, Zirconia and Ceria-Stabilized Zirconia Reinforced with Alumina Sites Subjected to Experimental Peri-Implantitis: A Preclinical Study in Dogs.Antibiotics (Basel). 2024 Jul 24;13(8):690. doi: 10.3390/antibiotics13080690. Antibiotics (Basel). 2024. PMID: 39199990 Free PMC article.
-
Influence of Section Thickness on the Accuracy and Specificity of Histometric Parameters Using Confocal Laser Scanning Microscopy in a Canine Model of Experimental Peri-Implantitis-A Proof of Concept.J Clin Med. 2023 Mar 23;12(7):2462. doi: 10.3390/jcm12072462. J Clin Med. 2023. PMID: 37048546 Free PMC article.
-
Histomorphometric Analysis of Osseointegrated Intraosseous Dental Implants Using Undecalcified Specimens: A Scoping Review.Biomimetics (Basel). 2024 Nov 3;9(11):672. doi: 10.3390/biomimetics9110672. Biomimetics (Basel). 2024. PMID: 39590244 Free PMC article.
References
-
- Albouy J.P., Abrahamsson I., Persson L.G., Berglundh T. Spontaneous progression of peri-implantitis at different types of implants. An experimental study in dogs. I: Clinical and radiographic observations. Clin. Oral Implant. Res. 2008;19:997–1002. doi: 10.1111/j.1600-0501.2008.01589.x. - DOI - PubMed
-
- Berglundh T., Persson L., Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002;29:197–212; discussion 232–233. doi: 10.1034/j.1600-051X.29.s3.12.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
