

Management of Filamentous Fungal Keratitis: A Pragmatic Approach
- PMID: 36294633
- PMCID: PMC9605596
- DOI: 10.3390/jof8101067
Management of Filamentous Fungal Keratitis: A Pragmatic Approach
Abstract
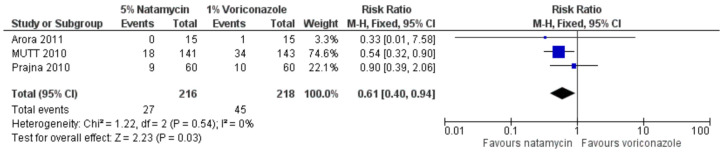
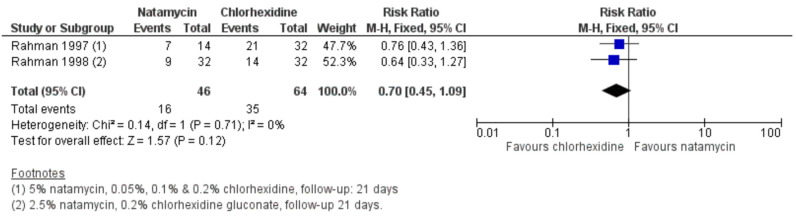
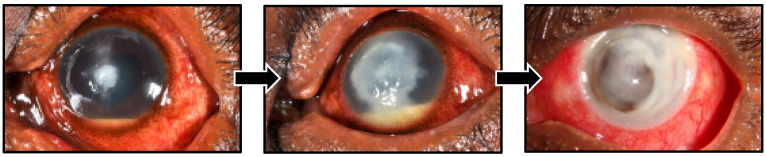
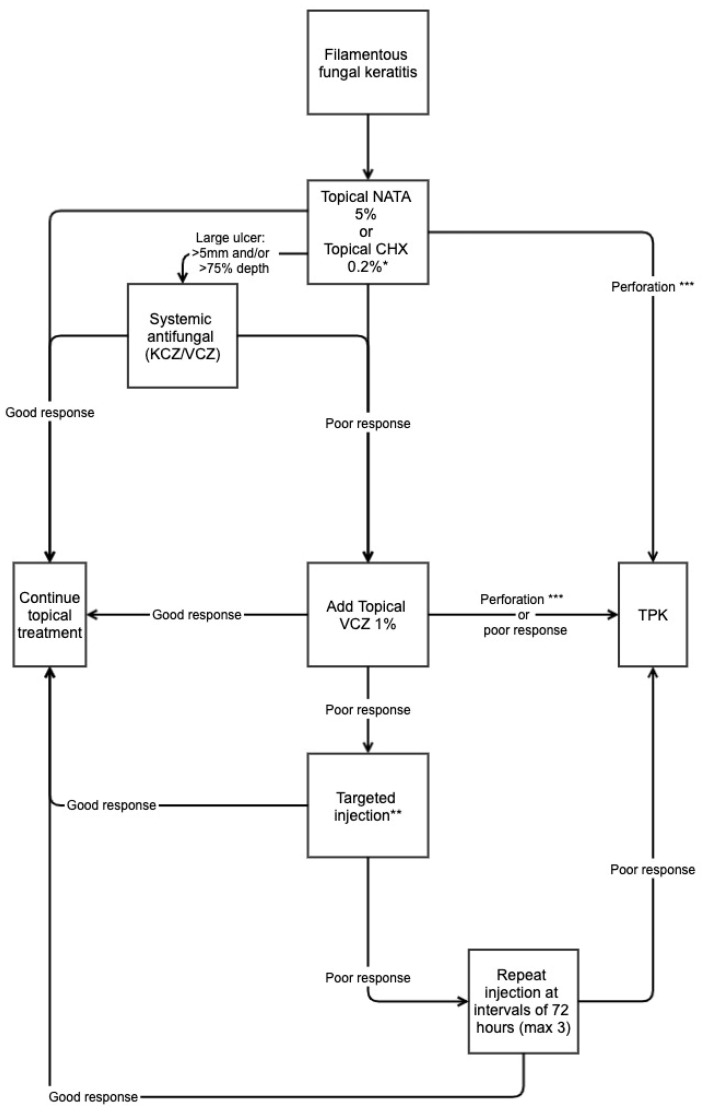
Filamentous fungal infections of the cornea known as filamentous fungal keratitis (FK) are challenging to treat. Topical natamycin 5% is usually first-line treatment following the results of several landmark clinical trials. However, even when treated intensively, infections may progress to corneal perforation. Current topical antifungals are not always effective and are often unavailable. Alternatives topical therapies to natamycin include voriconazole, chlorhexidine, amphotericin B and econazole. Surgical therapy, typically in the form of therapeutic penetrating keratoplasty, may be required for severe cases or following corneal perforation. Alternative treatment strategies such as intrastromal or intracameral injections of antifungals may be used. However, there is often no clear treatment strategy and the evidence to guide therapy is often lacking. This review describes the different treatment options and their evidence and provides a pragmatic approach to the management of fungal keratitis, particularly for clinicians working in tropical, low-resource settings where fungal keratitis is most prevalent.
Keywords: antifungals; chlorhexidine; fungal keratitis; management; microbial keratitis; microbiology; natamycin.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Patil A., Lakhani P., Majumdar S. Current perspectives on natamycin in ocular fungal infections. J. Drug Deliv. Sci. Technol. 2017;41:206–212. doi: 10.1016/j.jddst.2017.07.015. - DOI
-
- Borelli C., Schaller M., Niewerth M., Nocker K., Baasner B., Berg D., Tiemann R., Tietjen K., Fugmann B., Lang-Fugmann S., et al. Modes of action of the new arylguanidine abafungin beyond interference with ergosterol biosynthesis and in vitro activity against medically important fungi. Chemotherapy. 2008;54:245–259. doi: 10.1159/000142334. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
