

The Safety and Efficacy of Hepatic Transarterial Embolization Using Microspheres and Microcoils in Patients with Symptomatic Polycystic Liver Disease
- PMID: 36294764
- PMCID: PMC9605116
- DOI: 10.3390/jpm12101624
The Safety and Efficacy of Hepatic Transarterial Embolization Using Microspheres and Microcoils in Patients with Symptomatic Polycystic Liver Disease
Abstract
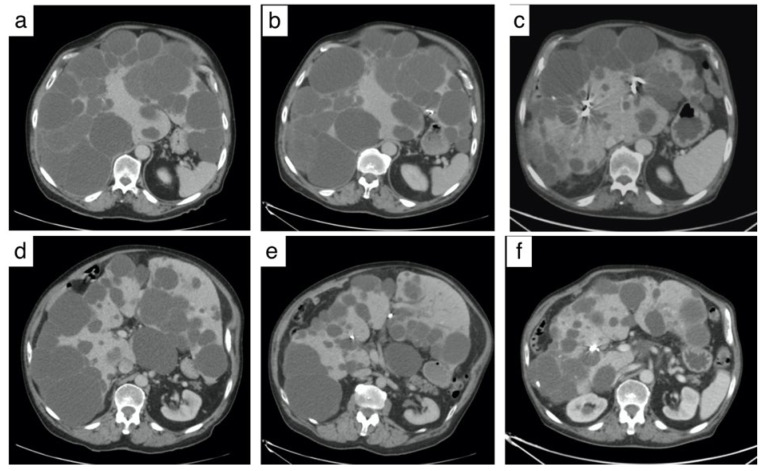
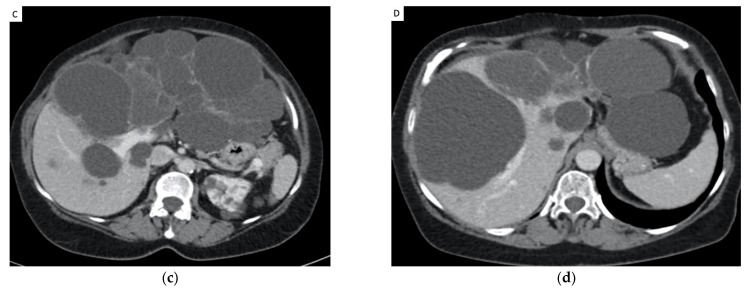
Purpose: We investigated the long-term safety and efficacy of hepatic transarterial embolization (TAE) in patients with symptomatic polycystic liver disease (PLD). Materials and Methods: A total of 26 patients were included, mean age of 52.3 years (range: 33−78 years), undergoing 32 TAE procedures between January 2012 and December 2019 were included in this retrospective study. Distal embolization of the segmental hepatic artery was performed with 300−500 µm embolic microspheres associated with proximal embolization using microcoils. The primary endpoint was clinical efficacy, defined by an improvement in health-related quality of life using a modified Short Form-36 Health Survey and improvement in symptoms (digestive or respiratory symptoms and chronic abdominal pain), without invasive therapy during the follow-up period. Secondary endpoints were a decrease in total liver volume and treated liver volume and complications. Results: Hepatic embolization was performed successfully in 30 of 32 procedures with no major adverse events. Clinical efficacy was 73% (19/26). The mean reduction in hepatic volume was −12.6% at 3 months and −27.8% at the last follow-up 51 ± 15.2 months after TAE (range: 30−81 months; both ps < 0.01). The mean visual analog scale pain score was 5.4 ± 2.8 before TAE and decreased to 2.7 ± 1.9 after treatment. Three patients had minor adverse events, and one patient had an adverse event of moderate severity. Conclusion: Hepatic embolization using microspheres and microcoils is a safe and effective treatment for PLD that improves symptoms and reduces the volume of hepatic cysts.
Keywords: efficacy; embolization; polycystic liver disease; safety.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Rosenfeld L., Bonny C., Kallita M., Heng A.E., Deteix P., Bommelaer G., Abergel A. Polycystic liver disease and its main complications. Gastroenterol. Clin. Biol. 2002;26:1097–1106. - PubMed
-
- Gigot J.F., Jadoul P., Que F., Van Beers B.E., Etienne J., Horsmans Y., Collard A., Geubel A., Pringot J., Kestens P.J. Adult polycystic liver disease: Is fenestration the most adequate operation for long-term management? Ann. Surg. 1997;225:286–294. doi: 10.1097/00000658-199703000-00008. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
