

Microaxial Left Ventricular Assist Device in Cardiogenic Shock: A Systematic Review and Meta-Analysis
- PMID: 36295065
- PMCID: PMC9605512
- DOI: 10.3390/life12101629
Microaxial Left Ventricular Assist Device in Cardiogenic Shock: A Systematic Review and Meta-Analysis
Abstract
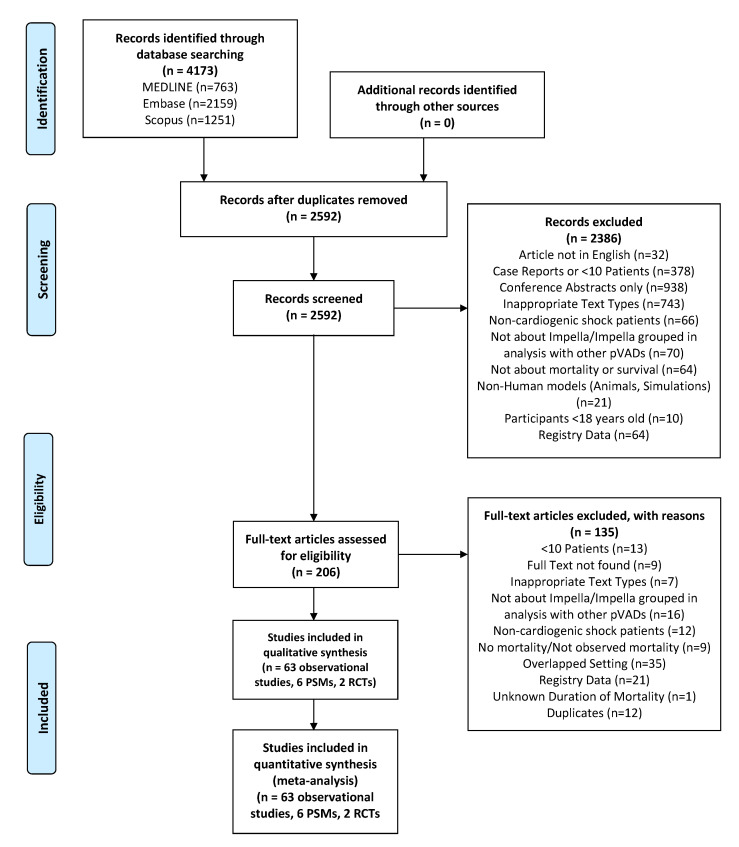
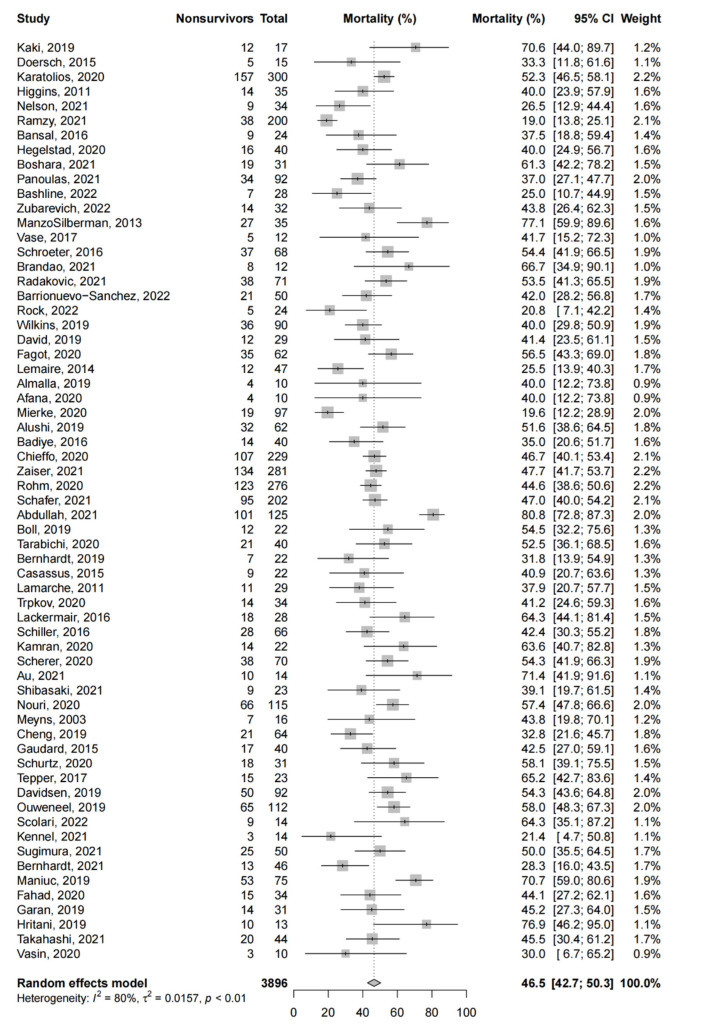
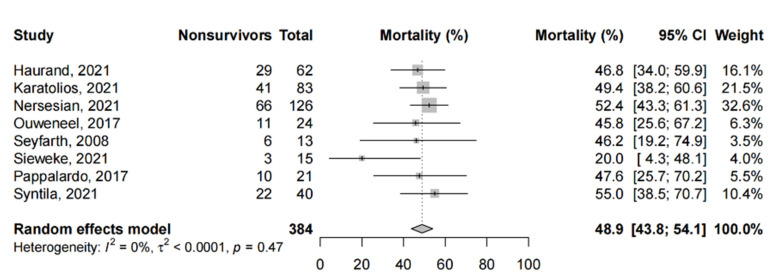
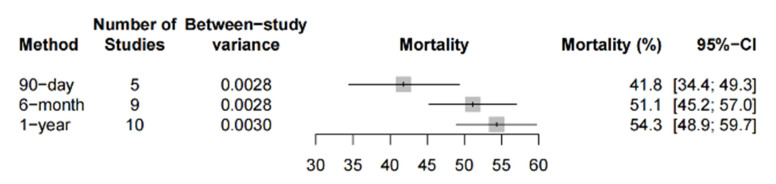
Microaxial left ventricular assist devices (LVAD) are increasingly used to support patients with cardiogenic shock; however, outcome results are limited to single-center studies, registry data and select reviews. We conducted a systematic review and meta-analysis, searching three databases for relevant studies reporting on microaxial LVAD use in adults with cardiogenic shock. We conducted a random-effects meta-analysis (DerSimonian and Laird) based on short-term mortality (primary outcome), long-term mortality and device complications (secondary outcomes). We assessed the risk of bias and certainty of evidence using the Joanna Briggs Institute and the GRADE approaches, respectively. A total of 63 observational studies (3896 patients), 6 propensity-score matched (PSM) studies and 2 randomized controlled trials (RCTs) were included (384 patients). The pooled short-term mortality from observational studies was 46.5% (95%-CI: 42.7-50.3%); this was 48.9% (95%-CI: 43.8-54.1%) amongst PSM studies and RCTs. The pooled mortality at 90 days, 6 months and 1 year was 41.8%, 51.1% and 54.3%, respectively. Hemolysis and access-site bleeding were the most common complications, each with a pooled incidence of around 20%. The reported mortality rate of microaxial LVADs was not significantly lower than extracorporeal membrane oxygenation (ECMO) or intra-aortic balloon pumps (IABP). Current evidence does not suggest any mortality benefit when compared to ECMO or IABP.
Keywords: Impella; cardiogenic shock; meta-analysis; ventricular assist device.
Conflict of interest statement
Kollengode Ramanathan serves as a co-chair of the Scientific Oversight Committee of the Extracorporeal Life support Organization (ELSO), and reports honoraria for educational lectures from Baxter Ltd., and Fresenius Ltd. All other authors declare no competing interest.
Figures
References
-
- Garcia-Garcia C., Rueda F., Oliveras T., Serra J., Labata C., Ferrer M., Bayes-Genis A. P779 Cardiogenic shock in STEMI patients: Prevalence, management and acute phase mortality over the last three decades. Eur. Heart J. 2018;39:ehy564.P779.
-
- Goldberg R.J., Spencer F.A., Gore J.M., Lessard D., Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: A population-based perspective. Circulation. 2009;119:1211–1219. doi: 10.1161/CIRCULATIONAHA.108.814947. - DOI - PMC - PubMed
-
- Baran D.A., Grines C.L., Bailey S., Burkhoff D., Hall S.A., Henry T.D., Hollenberg S.M., Kapur N.K., O’Neill W., Ornato J.P., et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock. Catheter. Cardiovasc. Interv. 2019;94:29–37. doi: 10.1002/ccd.28329. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
