

Comparison between Enteroscopy-, Laparoscopy- and Endoscopic Ultrasound-Assisted Endoscopic Retrograde Cholangio-Pancreatography in Patients with Surgically Altered Anatomy: A Systematic Review and Meta-Analysis
- PMID: 36295081
- PMCID: PMC9605390
- DOI: 10.3390/life12101646
Comparison between Enteroscopy-, Laparoscopy- and Endoscopic Ultrasound-Assisted Endoscopic Retrograde Cholangio-Pancreatography in Patients with Surgically Altered Anatomy: A Systematic Review and Meta-Analysis
Abstract
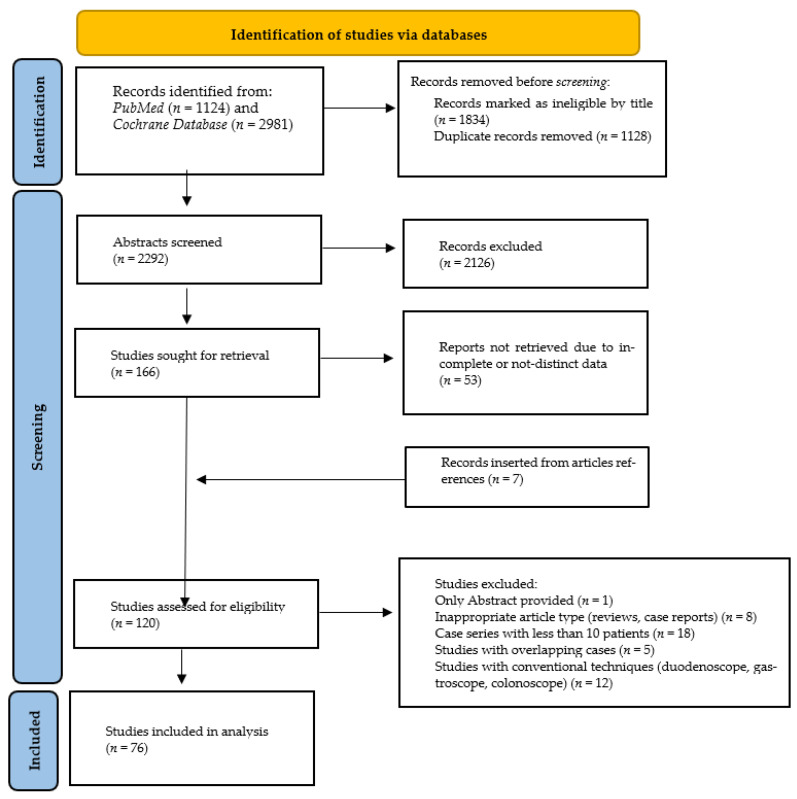
Background and aims: Endoscopic retrograde cholangiopancreatography (ERCP), in surgically altered anatomy (SAA), can be challenging and the optimal technique selection remains debatable. Most common foregut interventions resulting to this burden consist of Billroth II gastrectomy, Whipple surgery and Roux-en-Y anastomoses, including gastric by-pass. This systematic review, with meta-analysis, aimed to compare the rates of successful enteroscope-assisted (EA)-, endosonography-directed transgastric- (EDGE), and laparoscopy-assisted (LA)-ERCP.
Methods: A systematic research (Medline) was performed for relative studies, through January 2022. The primary outcome was technical success, defined as approaching the ampulla site. Secondary outcomes included the desired duct cannulation, successful therapeutic manipulations, and complication rates. We performed meta-analyses of pooled data, and subgroup analysis considering the EA-ERCP subtypes (spiral-, double and single balloon-enteroscope). Pooled rates are reported as percentages with 95% Confidence Intervals (95%CIs).
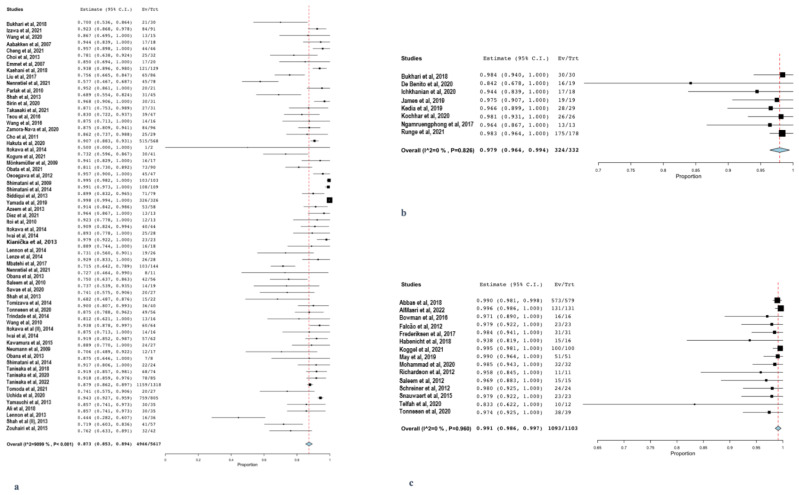
Results: Seventy-six studies were included (3569 procedures). Regarding primary outcome, EA-ERCP was the least effective [87.3% (95%CI: 85.3-89.4); I2: 91.0%], whereas EDGE and LA-ERCP succeeded in 97.9% (95%CI: 96.4-99.4; I2: 0%) and 99.1% (95%CI: 98.6-99.7; I2: 0%), respectively. Similarly, duct cannulation and therapeutic success rates were 74.7% (95%CI: 71.3-78.0; I2: 86.9%) and 69.1% (95%CI: 65.3-72.9; I2: 91.8%) after EA-ERCP, 98% (95%CI: 96.5-99.6; I2: 0%) and 97.9% (95%CI: 96.3-99.4) after EDGE, and 98.6% (95%CI: 97.9-99.2; I2: 0%) and 98.5% (95%CI: 97.8-99.2; I2: 0%) after LA-ERCP, respectively. The noticed high heterogeneity in EA-ERCP results probably reflects the larger number of included studies, the different enteroscopy modalities and the variety of surgical interventions. Comparisons revealed the superiority of LA-ERCP and EDGE over EA-ERCP (p ≤ 0.001) for all success-related outcomes, though LA-ERCP and EDGE were comparable (p ≥ 0.43). ERCP with spiral-enteroscope was inferior to balloon-enteroscope, while the type of the balloon-enteroscope did not affect the results. Most adverse events were recorded after LA-ERCP [15.1% (95%CI: 9.40-20.8); I2: 87.1%], and EDGE [13.1% (95%CI: 7.50-18.8); I2: 48.2%], significantly differing from EA-ERCP [5.7% (95%CI: 4.50-6.80); p ≤ 0.04; I2: 64.2%].
Conclusions: LA-ERCP and EDGE were associated with higher technical, cannulation, and therapeutic success compared to EA-ERCP, though accompanied with more adverse events.
Keywords: Billroth; EDGE; ERCP; RYGB; Roux-n-Y; balloon enteroscopy; enteroscopy; laparoscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Mishra T., Lakshmi K.K., Peddi K.K. Prevalence of Cholelithiasis and Choledocholithiasis in Morbidly Obese South Indian Patients and the Further Development of Biliary Calculus Disease After Sleeve Gastrectomy, Gastric Bypass and Mini Gastric Bypass. Obes. Surg. 2016;26:2411–2417. doi: 10.1007/s11695-016-2113-4. - DOI - PubMed
-
- Groot V.P., Rezaee N., Wu W., Cameron J.L., Fishman E.K., Hruban R.H., Weiss M.J., Zheng L., Wolfgang C.L., He J. Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2018;267:936–945. doi: 10.1097/SLA.0000000000002234. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
