

Treatment of Complex Two-Vessel Coronary Heart Disease with Single Left Internal Mammary Artery as T-Graft with Itself-A Retrospective Double Center Analysis of Short-Term Outcomes
- PMID: 36295575
- PMCID: PMC9610783
- DOI: 10.3390/medicina58101415
Treatment of Complex Two-Vessel Coronary Heart Disease with Single Left Internal Mammary Artery as T-Graft with Itself-A Retrospective Double Center Analysis of Short-Term Outcomes
Abstract
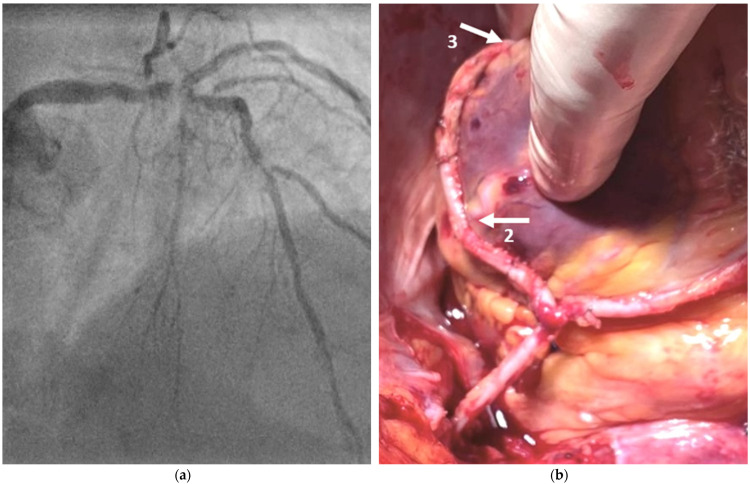
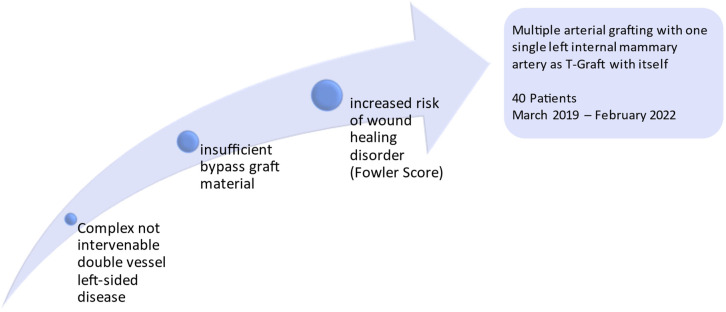
Background and Objectives: The strategy of revascularization may be constrained in patients with insufficient bypass grafts and with increased risk of wound healing disorders. Among those with complex left-sided double-vessel disease in whom a percutaneous coronary intervention (PCI), as well as the surgical procedure of minimally invasive coronary artery bypass grafting via left minithoracotomy (MICS CABG), is not a treatment option, CABG using the left internal mammary artery as a T-graft with itself may be an effective treatment strategy. Materials and Methods: We reviewed the data from patients treated in Cologne and Tuebingen from 2019 to 2022. We included 40 patients who received left internal mammary artery (LIMA) grafting, and additional T-graft with the LIMA itself. The objective was focused on intraoperative and short-term outcomes. Results: A total of 40 patients were treated with the LIMA-LIMA T-graft procedure with a Fowler score calculated at 20.1 ± 3.0. A total of 37.5% of all patients had lacking venous graft material due to prior vein stripping, and 21 patients presented severe vein varicosis. An overall of 2.6 ± 0.5 distal anastomoses (target vessels were left anterior descending, diagonal, intermediate branch, and/or left marginal ramus) were performed, partly sequentially. Mean flow of LIMA-Left anterior descending (LAD) anastomosis was 59.31 ± 11.04 mL/min with a mean PI of 1.21 ± 0.18. Mean flow of subsequent T-Graft accounted for 51.31 ± 3.81 mL/min with a mean PI of 1.39 ± 0.47. Median hospital stay was 6.2 (5.0; 7.5) days. No incidence of postoperative wound healing disorders was observed, and all patients were discharged. There was one 30-day readmission with a diagnosis of pericardial effusion (2.5%). There was no 30-day mortality within the cohort. Conclusions: Patients requiring surgical myocardial revascularization due to complex two-vessel coronary artery disease (CAD) can be easily managed with LIMA alone, despite an elevated Fowler score and a promising outcome. A prospective study needs to be conducted, as well as longer term surveillance, to substantiate and benchmark the long-term results, as well as the patency rates.
Keywords: LIMA; OPCAB; total arterial revascularization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Multiple Grafting with Single Left Internal Mammary Artery as T-Graft with Itself.Thorac Cardiovasc Surg. 2022 Oct;70(7):532-536. doi: 10.1055/s-0041-1731758. Epub 2021 Sep 14. Thorac Cardiovasc Surg. 2022. PMID: 34521140
-
Coronary Artery Revascularization with the Left Internal Mammary Artery (LIMA) to Diagonal (D) & Left Anterior Descending (LAD) Sequential and LIMA-LIMA "Y" Graft, Our Experiences at National Heart Foundation Hospital and Research Institute.Mymensingh Med J. 2020 Oct;29(4):939-944. Mymensingh Med J. 2020. PMID: 33116099
-
Use of the right internal mammary artery and the great saphenous vein for left anterior descending artery revascularization in patients whose left internal mammal artery cannot be used: a study based on transit-time flow measurement.J Cardiothorac Surg. 2020 Jun 5;15(1):126. doi: 10.1186/s13019-020-01172-5. J Cardiothorac Surg. 2020. PMID: 32503570 Free PMC article.
-
Spontaneous avulsion of left internal mammary artery graft a complication of coronary artery bypass surgery: case report and review of the literature.J Cardiothorac Surg. 2024 Sep 12;19(1):527. doi: 10.1186/s13019-024-03004-2. J Cardiothorac Surg. 2024. PMID: 39267103 Free PMC article. Review.
-
A Practical Approach to Hybrid Coronary Revascularization.Cardiol Rev. 2020 Sep/Oct;28(5):240-243. doi: 10.1097/CRD.0000000000000278. Cardiol Rev. 2020. PMID: 31985524 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
